Risk assessment
The risk to vulnerable consumers from Listeria monocytogenes in ready to eat smoked fish
This risk assessment considered three categories of vulnerable consumers; pregnant women, those aged over 65 and those who are considered immunocompromised due to a medical condition.
It is acknowledged that the risk to vulnerable consumers (those with weakened immune systems) from consuming food contaminated with Listeria monocytogenes is higher than that for the general population. This is because vulnerable consumers are more likely to suffer from invasive listeriosis, a form of the infection associated with severe symptoms and high mortality rates. Ready-to-eat (RTE) smoked fish has been implicated as the food vehicle in a number of recent outbreaks of listeriosis, and this risk assessment was commissioned to provide evidence to support a review of the advice to vulnerable consumers on consumption of RTE smoked fish.
This risk assessment considered three categories of vulnerable consumers:
- pregnant women (and unborn and newly delivered infants),
- those aged over 65
- those who are considered immunocompromised due to a medical condition or treatment.
A risk characterisation with corresponding uncertainties is provided for both hot and cold smoked RTE fish.
The risk assessment concluded that there was not enough evidence to distinguish the risk presented to the three identified groups of vulnerable consumers. It also identified that although the prevalence of L.monocytogenes was lower for hot-smoked than cold-smoked fish, that hot-smoked fish could not be considered risk-free, either due to ineffective smoking or, more likely, recontamination from contaminated processing equipment after the hot-smoking step.
On the basis of the evidence presented, we consider the frequency of occurrence of invasive listeriosis in the vulnerable population from consumption of cold smoked fish to be low (for example, rare but does occur) and hot smoked fish to be very low (for example, very rare but cannot be excluded).
We consider the severity of illness in the vulnerable population from L. monocytogenes infections to be high (for example, severe illness: causing life-threatening or substantial sequelae or illness of long duration).
The level of uncertainty around the frequency of listeriosis in the vulnerable population from consumption of hot or cold smoked fish was considered to be medium to reflect several key uncertainties, namely: the difficulty in estimating the infectious dose for L. monocytogenes and how it differs between different vulnerable groups; the long incubation period which can make attribution to a specific food vehicle difficult; the initial level of contamination and how it multiplies through the food chain; and consumer behaviour around use-by date and temperature abuse. The level of uncertainty for the severity of illness of listeriosis in the vulnerable population was considered to be low.
Listeria monocytogenes is a foodborne pathogen which can cause invasive listeriosis, an infection associated with severe symptoms and high mortality rates, in those with weakened immune systems. These individuals may be considered to be vulnerable consumers with regard to this pathogen. Certain ready-to-eat foods (foods that are not expected to undergo cooking or any other treatment which would inactivate bacterial contamination present) can be a particular problem if they have characteristics that support the survival and growth of Listeria monocytogenes. Smoked fish is recognised as one group of ready-to-eat foods which has been associated with listeriosis infections. This risk assessment has been requested to advise a review of the advice for vulnerable consumers on the risk of eating ready-to-eat smoked fish.
The evidence compiled in this risk assessment comes from industry and academic publications, as well as national and international reports and surveys of prevalence and incidents involving Listeria monocytogenes and illness in vulnerable consumers. The risk assessment considers the hazard of Listeria monocytogenes including the conditions that facilitate contamination, survival and growth in food, and the manifestation of listeriosis, the disease this bacterium can cause in humans. It gives details of outbreaks of disease associated with smoked fish, and the prevalence of the detection of Listeria monocytogenes in smoked fish which is available to the consumer. Finally, it also considers the production of smoked fish, and routes of contamination, or control steps that may limit the presence of the pathogen in the final product.
We concluded that the frequency (likelihood) of occurrence of invasive listeriosis in the vulnerable population from consumption of cold smoked fish is low (for example, rare but does occur), from the consumption of hot smoked fish is very low (for example, very rare but cannot be excluded) and that the severity of illness from listeriosis in the vulnerable population is high (for example, severe illness: causing life-threatening or substantial sequelae or illness of long duration).
We also highlighted a number of uncertainties where complete data were not available, for example, the dose of Listeria monocytogenes required to make a vulnerable consumer unwell.
Vulnerable consumers are defined as those individuals whose immune system is weakened and may be more susceptible to developing infection from L. monocytogenes (listeriosis) and likely to suffer more severe symptoms (FSA, 2018). For the purpose of this risk assessment, three groups of vulnerable consumers will be considered (FSA, 2018):
- Pregnant women, unborn and newly delivered infants
- Those aged over 65 years
- Those who are considered clinically vulnerable due to a medical condition or treatment which weakens their immune system. This includes cancer patients, patients undergoing immunosuppressive or cytotoxic treatment, people with diabetes, alcoholics (including those with alcoholic liver disease) and a variety of other conditions.
This risk assessment takes account of the most recent published information, data provided by UKHSA colleagues, and a risk assessment prepared by FSS in spring 2021 in response to a L. monocytogenes outbreak linked to smoked salmon. Additionally, to ensure consistency and efficiency, the Hazard Characterisation draws on the recent blue cheese and vulnerable consumers risk assessment (FSA, 2022).
Risk question
What is the risk to vulnerable consumers from Listeria monocytogenes in RTE smoked fish?
In scope
- risks from Listeria monocytogenes
- risks to the named vulnerable groups above
- risks from all types of smoked fish (for example, cold smoked and hot smoked fish)
Out of scope
- risks from other microorganisms that may be present in smoked fish including non-pathogenic strains of Listeria.
- risks from L. monocytogenes in smoked fish that is intended to undergo further treatment that would reduce or eliminate the microbiological load (for example cooking).
- risks to other groups, such as the immunocompetent population.
- risks from other smoked foods (for example smoked mussels, smoked cheeses).
- risk from pâté. All UK government guidance pages advise pregnant consumers to avoid all types of pâté (NHS, 2020; NHS 111 Wales, 2022; NHS Inform, 2022; NIDirect, 2022). Pâté is also covered in FSA and FSS guidance for healthcare and social care organisations (FSA, 2018; FSS, 2018).
- risks from other types of RTE fish product that may be hazardous to vulnerable consumers (for example raw unprocessed fish used in sushi-type dishes).
Additional considerations
Risks from salted cured fish, for example gravad
Gravad (also known as gravadlax or gravlax) is a cured fish product popular in Scandinavian countries (Lyhs et al., 2001). The process involves rubbing raw fish fillets with a mixture of sugar and salt and dill is added before a marinating step (Tham et al., 2000). In several outbreaks, cases reported consuming both smoked and gravad fish. Many of the data sets referred to in this risk assessment did not differentiate between smoked and gravad fish. Finally, it is unknown how popular or frequently available this particular product is in the UK market. For these reasons, gravad fish is considered in this risk assessment when the evidence includes it along with smoked fish, but salted and cured fish was considered out of scope. Therefore, data specific to this product was not sought in the preparation of this risk assessment and it is not included in the risk characterisation.
Key assumptions
Any contamination level could lead to illness in vulnerable consumers.
Dose-response models are developed on the assumption that a single organism could lead to infection (Pouillot et al., 2015). The probability of this occurring is incredibly small for healthy individuals but increases for vulnerable groups. As infectious dose would vary depending on the level of immune function in different vulnerable groups and there is little evidence available to calculate these different doses, the decision was made to treat the presence of any L. monocytogenes in smoked fish as a risk for vulnerable consumers.
Any strain of L. monocytogenes could lead to illness in vulnerable consumers.
There is growing evidence that different strains of L. monocytogenes exhibit differing abilities to cause infection (Abdelhamed et al., 2019; Farber et al., 2021), but there is not enough evidence to determine whether any strains pose more of a risk to vulnerable consumer compared to others. Regulation 2073/2005 (footnote 1) and UK Guidelines for Assessing the Microbiological Safety of Ready-to-Eat Foods Placed on the Market do not differentiate on risk of infection based on differences in L. monocytogenes strain (Health Protection Agency, 2009). Given this, this risk assessment considered the presence of any strain of L. monocytogenes in smoked fish to be capable of causing illness in vulnerable consumers.
Background
Over recent years there have been a number of incidents of listeriosis linked to smoked salmon and other types of smoked fish in the UK. Investigations of some of these incidents have not detected Listeria contamination that is above the legal threshold, however, cases of invasive listeriosis have been reported from people who are vulnerable to L. monocytogenes infection – including pregnant women and people with weakened immune systems – and there have been fatalities (information obtained by FSA and FSS from UKHSA as part of incident investigations).
At the time of writing, there is an ongoing incident of L. monocytogenes, with 12 cases reported (footnote 2) (9 England; 3 Scotland), with cases reported from October 2020 – February 2022. Eleven cases reported consumption of smoked fish, ten of which reported smoked salmon specifically. One pregnancy case is associated with this outbreak, and three of the cases are now deceased, with two patients having their death certificates recording L. monocytogenes as causative or contributory factors to their deaths.
In order to inform potential changes to advice for vulnerable consumers, FSS and FSA risk assessment teams have been asked to provide an assessment on what the risk to vulnerable consumers is from L. monocytogenes in RTE smoked fish.
Previous Risk Assessments
Several quantitative risk assessments specific to L. monocytogenes in smoked fish products have been published. Given the difficulty in determining the infective dose for L. monocytogenes (discussed below), most of these risk assessments did not break down the difference in risk for vulnerable groups compared to immunocompetent consumers. Lindqvist and Westöö calculated the probability of illness per serving comparing low-risk and high-risk groups (including children <1 year, pregnant women, those aged over 65 years, and those with HIV/AIDS) using data from Sweden (Lindqvist and Westöö, 2000). The mean probability of illness per serving was 2.0×10-3 for the low-risk group compared to 1.6×10-2 for the high-risk group (Lindqvist and Westöö, 2000); this equates to the high-risk group having an 8-fold increase in risk of acquiring infection from smoked fish. The authors acknowledge their model for calculating dose-response was conservative, resulting in an overestimation of predicted L. monocytogenes case numbers compared to actual numbers recorded in Sweden. They further reflected that since the extent of underreporting of listeriosis is unknown, it is impossible to estimate how closely their predictions might reflect true case numbers (Lindqvist and Westöö, 2000). Pouillot et al. broke down the mean risk of contracting invasive listeriosis per serving of cold-smoked salmon in France (Pouillot et al., 2009); their results are reproduced in
Table 1. Their results also found an increased risk of acquiring listeriosis from consuming smoked fish for vulnerable subpopulations compared to the overall population.
Table 1. The mean risk of contracting invasive Listeriosis per serving of cold-smoked salmon in France (taken from Pouillot et al., 2009)
| Subpopulation | Mean risk per serving [95% Credibility Interval] | Increase in risk compared to immunocompetent |
|---|---|---|
| Pregnant | 1.4 x 10−5 [4.3 x 10−7, 5.5 x 10−4] | x140 |
| Susceptible (immunocompromised) | 5.4 x 10−6 [1.7 x 10−7, 2.2 x 10−4] | x54 |
| Over 65 years | 1.3 x 10−6 [4.1 x0−8, 5.3 x 10−5] | x13 |
| Reference (immunocompetent) | 1.0 x 10−7 [3.3 x 10−9, 4.3 x 10−6] | - |
| Overall | 7.8 x 10−7[2.5 x 0−8, 3.1 x10−5] | - |
*Defined as the subpopulation of individuals with one of the following risk factors: cancer (all types), dialysis, transplant, liver cirrhosis, AIDS, and diabetes (all types), regardless of age
Two quantitative risk assessments have been produced to assess the risk from L. monocytogenes in several RTE products: one from the FDA/FSIS in 2003 and one from the WHO/FAO in 2004 (FDA, 2003; WHO, 2004). Both considered the risk from smoked seafood specifically amongst other RTE products associated with L. monocytogenes infections. Out of 23 RTE products, the FDA risk assessment ranked smoked seafood high risk, (5 out of 23) for risk of infection on a per serving basis. It was ranked number 9 out of 23 (moderate risk) on a predicted median case number per annum basis, taking into account either that a small percentage of consumers regularly consume the product or consumption is infrequent and portions small. The FDA’s “smoked seafood” category included both hot- and cold-smoked fish and other seafood like smoked mussels and oysters. In the WHO assessment, cold-smoked fish had the highest estimated cases of listeriosis per serving compared to three other RTE products, at 0.053 cases per 1 million servings. It had the second highest estimated risk per consumer, after pasteurised milk. The WHO risk characterisation data is summarised in Table 2.
Table 2. WHO risk characterisation data for various ready-to-eat foods (taken from (WHO, 2004)
| Food | Cases of listeriosis per 10 million people per year | Cases of listeriosis per 1 million serving |
|---|---|---|
| Pasteurised milk | 9.1 | 0.005 |
| Ice cream | 0.012 | 0.000014 |
| Cold-smoked fish | 0.46 | 0.053 |
| Fermented meat products | 0.00066 | 0.0000021 |
-
Regulation 2073/2005 is used throughout this document as shorthand for Retained EU Regulation (EC) 2073/2005 which applies in England, Wales and Scotland and EU Regulation (EC) 2073/2005 which applies in Northern Ireland.
-
Two further cases within this cluster were identified while the risk assessment was in preparation. The number total of cases as of June 2022 is 14, 11 in England and 3 in Scotland.
Listeria monocytogenes is a ubiquitous Gram-positive bacterium which occurs naturally in terrestrial and aquatic (fresh and salt water) environments (Thomas et al., 2012). Smoked fish has been identified as a vehicle for L. monocytogenes due to a combination of specific factors including a relatively high prevalence of initial contamination on fish, processing which may not fully eliminate contamination which is present, a production process with multiple opportunities for contamination or recontamination and a final product which can support the growth of the bacterium over its relatively extended shelf life (FAO and WHO, 2006; Ricci et al., 2017).
Listeriosis is an illness that is caused by infection with the bacterium L. monocytogenes, and while it usually presents as self-limiting mild gastroenteritis in immunocompetent people, it can cause serious illness (invasive listeriosis) in vulnerable people such as people aged over 65, pregnant women and those with impaired immunity (Thomas et al., 2012). The difficulty in eliminating L. monocytogenes from RTE products which can support its growth, and the very low relative risk to the population as a whole, is recognised in the Microbiological Criteria for Foodstuffs Regulation 2073/2005 which states that businesses must demonstrate that L. monocytogenes will not exceed the limit of 100 CFU/g throughout shelf life or, where the FBO is unable to demonstrate to the satisfaction of the Competent Authority that the product will not exceed 100 CFU/g at the end of shelf life, absence in 25 g before the product has left the immediate control of the FBO. A number of techniques can be used to determine shelf life, including shelf-life studies and historical data, predictive (computer) modelling and challenge testing. Any studies must be carried out using realistic parameters that the food will be subjected to, including the conditions during manufacture, transport, retail and in the consumer’s home.
There are 17 species in the genus Listeria with two (L. monocytogenes and L. ivanovii) considered pathogens of any species (Orsi and Wiedmann, 2016). L. ivanovii is generally considered a pathogen of ruminants which may opportunistically infect humans, whereas L. monocytogenes is an important human foodborne pathogen (Guillet et al., 2010; Orsi and Wiedmann, 2016). As well as environmental testing for L. monocytogenes, businesses may also test for Listeria spp. in their processing environment as an indicator organism to ensure the efficacy of their cleaning protocol (Thomas et al., 2012; Townsend et al., 2021).
Microbial description
L. monocytogenes is a species of Gram positive, facultatively anaerobic, rod-shaped bacteria, which are non-spore forming. It can grow over a wide range of temperatures (-0.4 – 50°C) (Farber and Peterkin, 1991). There are many reservoirs of L. monocytogenes, as it can infect and cause listeriosis in ruminants (Walland et al., 2015) and, unlike many other foodborne pathogens, can live and grow in the natural environment without the need to grow within an animal host (Chasseignaux et al., 2001). Environmental cross-contamination is a major issue with respect to L. monocytogenes. It can occur through direct contact with raw materials, personnel, aerosols and contaminated utensils, equipment, etc. Cross-contamination can occur at any step where the product is exposed to the environment, including processing, transportation, retail, catering and in the home. L. monocytogenes is tolerant to various environmental conditions, such as low oxygen, refrigeration temperatures (even freezing temperature -20°C), high salt (NaCl up to 10%) or acidity (pH ≤ 4 to 5) which results in survival for long periods (up to years) in the environment, on foods, in the processing plant, and in household refrigerators (Miller, 1992; Liu et al., 2005).
L. monocytogenes is a human foodborne pathogen, with infection by L. monocytogenes known as listeriosis. Foodborne listeriosis is a relatively rare illness in comparison to other foodborne diseases (see Table 3); however, the outcomes of illness can be serious with high fatality rates reported (PHE, 2018; PHS, 2020). Listeriosis mainly affects vulnerable groups such as immunosuppressed people, infants and pregnant women (and their unborn children). Levels of miscarriage are around 30%, but a L. monocytogenes infection can be asymptomatic in the pregnant person.
Table 3. Listeriosis cases in UK, 2018-2020 (personal communications with Epidemiology in Foodborne Infections Group “Report of Annual Human Infection Data for 2020”)
| Nation | Case/rate | 2018 | 2019 | 2020 |
|---|---|---|---|---|
| England | Cases | 151 | 142 | 116 |
| England | Rate | 0.27 | 0.25 | 0.21 |
| Wales | Cases | 6 | 3 | 7 |
| Wales | Rate | 0.19 | 0.10 | 0.21 |
| Scotland | Cases | 12 | 6 | 13 |
| Scotland | Rate | 0.22 | 0.11 | 0.24 |
| Northern Ireland |
Cases |
3 | 5 | 6 |
| Northern Ireland | Rate | 0.16 | 0.26 | 0.32 |
| United Kingdom | Total cases | 172 | 156 | 142 |
| United Kingdom | Rate | 0.26 | 0.23 | 0.21 |
*per 100,000 population. Population data are ONS mid-year estimates.
Disease characterisation
Various clinical manifestations are associated with L. monocytogenes infection, and these can be grouped in two categories: invasive and non-invasive listeriosis. Non-invasive listeriosis typically occurs in immunocompetent individuals, it has been observed during outbreaks where the majority of cases develop symptoms of gastroenteritis, such as diarrhoea, fever and headache, after a short period of incubation, as described by Aureli et al. (2000). Non-invasive listeriosis has not been well-studied as the clinical presentations do not typically warrant medical intervention and are therefore not identified as testing is unlikely to take place. Additionally, it is difficult to culture Listeria in stool samples, which may limit the detection of non-invasive listeriosis. There is no data available to define the number or proportion of cases of non-invasive listeriosis that occur in the populations considered vulnerable in this risk assessment, however, there is some evidence of vulnerable individuals being identified in investigations into outbreaks of non-invasive listeriosis, for example over 65 year olds in Dalton et al., 1997. Non-invasive listeriosis is typically self-limiting and symptoms only last a few days (Aureli et al., 2000). According to Warriner and Namvar non-invasive listeriosis is associated with an intake of high levels of L. monocytogenes (>1000 CFU/g) (Warriner and Namvar, 2009), which is also supported by assessment carried out by EFSA (EFSA, 2018) and this may reflect the suspected under reporting of non-invasive listeriosis in immunocompetent individuals who are unlikely to seek medical support.
Invasive listeriosis typically occurs in vulnerable or immunocompromised individuals. The symptoms of invasive listeriosis are severe, and include fever, myalgia (muscle pain), septicaemia, and meningitis. The incubation period is usually one to two weeks but can vary from between a few days to 90 days (WHO, 2018; Johnsen et al., 2010). The long incubation period creates difficulty in identifying the food vehicle responsible for infection, although the adoption of whole genome sequencing has improved the ability to link individual cases to outbreaks, which had previously been more challenging. Anyone can become ill from L. monocytogenes infection, but those aged over 65, pregnant women, unborn and new-born babies and otherwise immunocompromised persons can be considered higher-risk groups as they are more likely to acquire listeriosis from L. monocytogenes contaminated food, and subsequently this infection is more likely to be invasive compared to the immunocompetent population (see section 3.2). The case fatality rate of invasive listeriosis is high, ranging from 20 - 30% (Mead et al., 1999; PHE, 2017, 2018, 2021). Pregnant women infected with L. monocytogenes can experience miscarriage, stillbirth and premature birth which, while not typically fatal for the mother, can be fatal for the foetus or baby (Pezdirc et al., 2012).
Presentation of Listeriosis
L. monocytogenes is a cause of acute, self-limited, febrile gastroenteritis in immunocompetent persons. Invasive listeriosis causes severe acute (and sometimes fatal) illness, and post-listeriosis sequelae such as neurological symptoms can persist chronically (Drevets and Bronze, 2008). In addition, there are findings that some L. monocytogenes are able to colonise and persist in the gallbladder, which suggests the occurrence of long-term and chronic infections and demonstrates the ability of pathogenic Listeria spp. to survive within the various microenvironments of the gastrointestinal tract for a long period (Gahan and Hill, 2005). Although rare, L. monocytogenes infections can also affect bone, joints and sites in the chest which could develop into chronic disease (Bader, Al-Tarawneh and Myers, 2016).
We could not find a recent estimation of the underreporting of listeriosis cases in the UK, but Adak et al. (2002) put a factor of two for the number of cases and those not reported. It is also noted that L. monocytogenes is a schedule 2 causative agent which it is mandatory to report (Adak, Long and O’Brien, 2002). This should mean that any detected cases are reported, and that only undetected cases are likely to remain unreported.
Infective Dose
Quantitative assessments indicate that among immunocompetent adults, exposure to high doses of L. monocytogenes in foods is required to cause febrile gastroenteritis. Additionally, EFSA modelling suggests that 90% of invasive listeriosis cases are caused by ingestion of RTE foods containing > 2000 CFU/g (EFSA, 2018). Levels under 100 CFU/g in food at point of consumption (for example the legal limit at the end of shelf life) are regarded as safe, meaning that people consuming foods with low levels of L. monocytogenes have an extremely low risk of contracting listeriosis (EFSA, 2013, 2014, 2018). Nevertheless, as with all disease-causing microorganisms, there is no threshold below which there is a true “zero” risk for human illness. Epidemiological data has indicated that doses as low as 8 CFU/g of L. monocytogenes can cause listeriosis (Pouillot et al., 2016), although it is recognised that further data is required to further inform understanding of infective dose and probability of infection in vulnerable populations (Farber et al., 2021). In ready-to-eat (RTE) products intended for infants and for special medical purposes, there must be absence of L. monocytogenes in samples of 25g throughout shelf-life (EFSA, 2018). In other RTE foods that can support the growth of L. monocytogenes (including smoked fish) the bacterium must not be present in 25 g of sample when leaving the production plant, or the business must demonstrate that the product will not exceed the limit of 100 CFU/g throughout its shelf life.
Dose-response data from human volunteer studies with L. monocytogenes or from volunteer studies with a surrogate pathogen do not exist. In 2018, EFSA conducted a risk assessment on “Listeria monocytogenes contamination in RTE food and the risk for human health”. This risk assessment states that the average probability of a single L. monocytogenes CFU to cause illness in a specific host (the r value), reflects the strain virulence and host susceptibility, and ranges three orders of magnitude, from the least (for example under 65 years old without underlying condition) to the most susceptible (for example immunocompromised) populations. Reported r values for specific outbreaks with highly susceptible populations increased the range by another five orders of magnitude. Thus, the probability of a single bacterium to cause illness may range 100 million times depending on variability in host susceptibility and L. monocytogenes virulence (EFSA, 2018). It is recognised that uncertainty in most dose-response models results from a lack of data on the impact on highly susceptible populations from low level exposure (Farber et al., 2021). As a result, there is no single value for infectious dose. In earlier dose response modelling work, Pouillot et al. (2015) reviewed available literature and estimated that the relative risk of invasive listeriosis for pregnant women was 100 times higher than for non-pregnant women, and that relative risk levels more than 1000 times higher than that for the <65 year old general population have been reported for individuals with chronic lymphocytic leukaemia (Pouillot et al., 2015). This data is broadly similar to that reported in section 1.3 from previous risk assessments, but it does indicate the uncertainty in the understanding of infectious dose. For example, Pouillot et al. (2009) reported that the mean risk of contracting invasive listeriosis for susceptible (immunocompromised) individuals is x 54, but Pouillot et al. (2015) reported a risk level of more than x 1000 for a specific medical condition. Similarly, the WHO technical report on L. monocytogenes in ready-to-eat foods calculated susceptibilities ranging from x 7.5 to x 2,500 for different vulnerable groups compared to the reference population of under 65 years in age with no other medical conditions (WHO, 2004).
Previous outbreaks
To identify outbreaks associated with L. monocytogenes and smoked fish, a literature search was performed. Pubmed and Scopus were searched using the search terms “listeri* AND outbreak AND ("smoked fish" OR "smoked salmon" OR "smoked trout" OR "smoked mackerel" OR kipper)” with no restriction on language or date of publication. Google scholar was also searched, reviewing the first 100 hits sorted on relevance. Public health websites from the CDC, EFSA and the four UK nations were also searched.
A total of eight outbreaks were identified from the literature search (Table 4). Case numbers ranged from 4 cases up to 27 cases. In the 6 outbreaks that provided sufficient detail on the types of cases, vulnerable groups were a majority of the cases in 5 of them. Where it was specified, all the outbreaks were due to cold-smoked fish products.
Table 4. Outbreaks associated with L. monocytogenes contamination of smoked fish
| Years/location | Number of cases (deaths) | Vulnerable groups affected | Product | References |
|---|---|---|---|---|
| August 1994 to June 1995 Sweden | 9 (1) |
5 elderly 3 pregnancy 1 clinically vulnerable |
Cold smoked gravad rainbow trout | Ericsson, 1997, Tham et al., 2000 |
| 1997 Finland | 5 (0) |
1 pregnancy All cases from known risk group |
Cold smoked halibut and trout | Miettinen et al., 1999, Nakari et al., 2014 |
| May 2013 to September 2015 Denmark | 10 (3) |
1 pregnancy All cases from known risk group |
Cold smoked halibut and trout | Gillesberg Lassen et al., 2016 |
| June 2013 to September 2015 Denmark | 10 (4) | All cases from known risk group | Cold smoked salmon | Gillesberg Lassen et al., 2016 |
| 2013 to 2015 Sweden | 27 (NA*) | NA | Gravad and smoked fish | Lopez-Valladares Danielsson-Tham and Tham, 2018 |
| July 2014 to February 2019 EU | 22 (5) | Median age of outbreak cases 76 years, interquartile range 64 to 83 | Cold smoked or gravad salmon and cold smoked trout | EFSA and ECDC, 2019 |
| October 2015 to May 2018 EU | 12 (4) | 9 elderly | Cold smoked salmon | Schjørring et al., 2017; EFSA and ECDC, 2018 |
| 2020 UK | 4 (2) |
3 clinically vulnerable 1 pregnancy |
Smoked salmon^ | EFSA, 2020, UKHSA personal communication |
* NA details not provided in reference
^ Further details on smoking process unavailable
Given the low case numbers and the extended incubation period, historically it has been difficult to identify L. monocytogenes outbreaks. This was highlighted by a recent paper which made use of sequencing data from German clinical and food isolates to link cases to food exposures (Lachmann et al., 2022). This analysis retrospectively identified 22 outbreaks in Germany attributed to L. monocytogenes in smoked fish between 2010 and 2021. These outbreaks were associated with 228 cases, with a median age of 78 years, and involved 50 deaths, of which 17 were confirmed to have died from listeriosis. The results estimated that 27% of all listeriosis cases in Germany between 2018 and 2020 were likely due to L. monocytogenes contamination of smoked or gravad salmon products (Lachmann et al., 2022).
UK Food Safety Incidents involving L. monocytogenes and Smoked Fish
A food safety incident is defined as any event where, based on the information available, there are concerns about confirmed or suspected risks to the safety, quality, or integrity of food and/or feed that could require intervention to protect consumers’ interests (FSA, 2021). Incidents are usually notified to FSA or FSS if they concern a serious localised food hazard, if they are likely to affect a vulnerable population or if the food is distributed in an area encompassing more than one Local Authority/Local Council; it does not necessarily mean a clinical case of foodborne illness was associated with the incident. Microbiological incidents recorded by the FSA and FSS for the time period of 2015 – 2019 were investigated for those relating to L. monocytogenes in smoked fish. Out of 1,734 incidents, 18 were due to L. monocytogenes in smoked fish, meaning 1.0% of all incidents in this time period could be attributed to this specific pathogen and food product combination (Table 5). All recorded incidents in Table 5 involved smoked salmon as opposed to other types of smoked fish.
Table 5. Incidents reported to the Food Standards Agency and Food Standards Scotland involving L. monocytogenes in smoked fish, 2015 - 2019
| Year | Microbiological incidents | L. monocytogenes incidents | L. monocytogenes and smoked fish incidents |
|---|---|---|---|
| 2015 | 290 | 29 | 1 |
| 2016 | 302 | 34 | 6 |
| 2017 | 380 | 49 | 2 |
| 2018 | 358 | 39 | 6 |
| 2019 | 381 | 63 | 3 |
Due to changes in recording and accessing incidents data, data for the years 2020-2022 was extracted differently than for previous years. Table 6 provides the number of L. monocytogenes in smoked fish incidents recorded by the FSA and the FSS for these years.
The number of food incidents per year in the UK ranged from 1 to 6. In all but one instance where the fish species was recorded, smoked salmon was the source of L. monocytogenes contamination.
Table 6. Incidents reported to the Food Standards Agency and Food Standards Scotland involving L. monocytogenes in smoked fish, 2020 - March 2022
| Year | L. monocytogenes and smoked fish incidents |
|---|---|
| 2020 |
4 (2 salmon, 2 species not defined) |
| 2021 | 6 (4 salmon, 1 smoked salmon pâté, 1 speciies not defined) |
| 2022 | 4 (3 salmon, 1 trout) |
UK Listeriosis cases associated with Smoked fish
This section was provided by the UKHSA from their records relating to listeriosis, and therefore an incident in this section refers to cases or outbreaks of listeriosis.
All cases of listeriosis reported in England are requested to complete a food history questionnaire, asking about food exposures in the 30 days prior to illness onset (UK Health Security Agency). This questionnaire includes questions around smoked fish consumption and location of purchase. Where L. monocytogenes from multiple cases match by analysis of WGS results, food exposures can be compared to identify similarities between cases, which allows potential vehicles of interest to be further investigated to uncover the source of the outbreak. However, the most common way to initially identify likely food sources is by the unrelated examination of foods as part of Local Authority routine food inspections and the matching by WGS analysis of food or environmental L. monocytogenes to those from cases of human listeriosis, sometimes several years apart. Due to the sensitivity and specificity of analysis of WGS data, where there is a match to a non-human isolate, food exposure information and traceback can identify a likely source of contamination, even in instances where there is only one case.
As of 11 March 2022, data from investigations into outbreaks and single cases matching food isolates identified by WGS in UKHSA have identified a total of seven incidents that have been linked to smoked fish from 2015 - 2022 through microbiology and epidemiological evidence (see Table 7). Between 2015 - 2019, there were an additional three incidents, leading to 5 cases and 3 deaths, that were potentially linked to smoked salmon by microbiology (WGS) without corroborating epidemiological or food chain traceback data.
From 2015-2019, there were 3 incidents involving a total of 3 cases, with one case each linked to smoked fish via microbiological and epidemiological evidence. From 2020-March 2022 there were 4 incidents involving a total of 16 cases. Despite covering less than half of the same time period, the 2020-2022 period resulted in 5 reported deaths and 2 pregnancy-associated cases, compared to 1 death and 1 pregnancy associated case in 2015-2019. This suggests an increase in the number of cases associated with smoked fish consumption, number of deaths and number of pregnancy-associated cases in 2020- March 2022 as compared to 2015-2019, but it is not known if there were any differences in consumption volumes or frequency in the population between these two time periods. However, this pattern is not represented as strongly in the FSA/FSS food incident data.
Table 7. Summary of L. monocytogenes incidents and cases from 2015-2019 and from 2020-present with microbiological and epidemiological evidence implicating smoked fish as the vehicle of infection
| Year period | Incidents | Cases | Size of incidents (average range) | Deaths | Pregnancy associated cases | Fish species/products |
|---|---|---|---|---|---|---|
| 2015 to 2019 | 3 | 3 | 1 (1 case each) | 1 | 1 | 1 smoked salmon, 1 salmon pâté, 1 smoked mackerel |
| 2020 to March 2022 | 4* | 16 | 4 (1 to 10) | 5 | 2 | 4 smoked salmon^ |
*Includes the ongoing national outbreak of L. monocytogenes related to smoked fish. Data correct to March 2022.
^Four independent incidents, involving 4 different suppliers of smoked fish.
In determining the risk characterisation consideration was given to whether any differentiation could be made between different vulnerable groups, different smoking techniques or different species of fish. These are detailed below along with a summary on the risk of listeriosis in relation to smoked fish consumption.
Effect on different vulnerable groups
Initially this risk assessment aimed to examine the risk of listeriosis in three separate vulnerable groups: pregnant women and unborn and newly delivered infants, those aged over 65, and those who are considered clinically vulnerable due to a medical condition or treatment which affects their immune system. A number of significant outbreaks (between 4 and 22 cases in each) associated with L. monocytogenes contamination of smoked fish were detailed in Table 4. Not all of these provided sufficient detail to ascertain if affected cases came from the vulnerable groups included in this risk assessment, but where this information was provided, vulnerable groups were the majority or all of cases. However, the data available for these outbreaks did not provide enough evidence to differentiate between the risk for different vulnerable groups. It is also noted that only more serious cases of listeriosis are likely to be detected, and that those in vulnerable groups may also suffer from non-invasive listeriosis which is not reported. It should be noted that the risk to pregnant consumers is linked to the risk of miscarriage, stillbirth or premature birth from listeriosis, and that listeriosis may be asymptomatic or associated with mild symptoms in the mother.
Although the increased risk of listeriosis to vulnerable groups was highlighted by all the literature consulted as part of this risk assessment, it was not possible to identify a specific infectious dose for vulnerable consumers more generally, or broken down by the categories outlined above. The risk reported in publications ranged from 10 to 100 times higher than the immunocompetent population, and even up to 1000 times in the case of one specific medical condition.
Non-invasive listeriosis typically occurs in immunocompetent individuals and is not well-studied as clinical presentation is rare. Invasive listeriosis typically occurs in vulnerable or immunocompromised individuals, the symptoms are severe and hospitalisation is required in a high number of cases. For these reasons, the risk characterisation in this risk assessment deals specifically with invasive listeriosis.
In summary, although it is recognised that the risk may differ between these different vulnerable groups, the data presented here supports the conclusion that the risk is higher than for the general population for all of these groups, and that while the immunocompetent population may be able to safely consume food contaminated with L. monocytogenes to a level within the legal limit, no level of L. monocytogenes contamination can be considered safe for vulnerable groups. Although it is not possible to determine the level of L. monocytogenes contamination which can be considered safe for vulnerable groups as a specific infectious dose, there is information available to show that this level is likely to be significantly lower than the level required to cause illness in immunocompetent groups.
Effect of smoking techniques
The data presented in this risk assessment demonstrates that if adequate protocols are used, cold smoking and the associated processing can significantly reduce levels of L. monocytogenes in fish if the initial contamination is in line with anticipated levels of natural contamination. Hot smoking at the necessary temperature can inactivate the pathogen. However, all producers use slightly different procedures and this may affect the efficacy of either hot or cold smoking as a control. Prevalence data suggests that likelihood of contamination in hot smoked fish may be a third to an eighth of that in cold smoked fish. We note that the data available to allow the comparison of hot and cold smoking was incomplete as a number of authors reporting prevalence of L. monocytogenes did not define what type of smoking had been used. Additionally, there was not enough data available to compare the reported level of contamination between hot and cold smoked fish products. The further processing that these RTE products are subject to post either hot or cold smoking may introduce or re-introduce L. monocytogenes contamination, and the prevalence data presented demonstrates that neither hot nor cold smoked fish can reliably be considered free of L. monocytogenes. The outbreak data presented in section 3.3 does not include any reported incidents attributed to hot smoked salmon.
Although the limited data and uncertainties around the differences in production practices used by different FBOs lead to certain gaps in our understanding of the difference in risk between hot smoked and cold smoked fish, we believe the prevalence and outbreak data support the separate consideration of hot and cold smoked fish in the risk conclusion.
Effect of species of fish
A number of different species of smoked fish are available to UK consumers. The prevalence data presented in this risk assessment suggests that L. monocytogenes contamination can be found in any RTE smoked fish product, although reports from different authors implicated different fish species as more likely to be contaminated. For this reason, we do not think there is sufficient data to differentiate between smoked fish of different species. However, it is worth noting, that the most abundantly available evidence used throughout this RA concerns smoked salmon products, which likely to reflect the species preference of UK consumers, with salmon representing 46.6% of the UK chilled seafood species value share in 2021, and smoked salmon making up around a quarter of chilled salmon sales (Chilled Seafood in Multiple Retail, 2021).
Effect of growth within product
Modelling work presented in this risk assessment suggested that typical consumer behaviour could allow low levels of contamination (1 CFU/g) in product with average pH and aw to multiply to above the legal limit of 100 CFU/g by the end of shelf life. However, the model does not take into account the effect of smoke or other inhibitory substances that L. monocytogenes may be exposed to, or the effect of other lactic acid bacteria present within the product. Thus modelling alone cannot give a true indication of levels likely to occur at the end of shelf life. Additionally, industry practice may also help to limit the potential for L. monocytogenes to be present in a final product. For example, we understand from colleagues in the FSS Incident Investigations and Enforcement Delivery Teams, that it is common industry practice to demonstrate no detection of L. monocytogenes in 25 grams at the beginning of shelf life. Where L. monocytogenes has been detected in 25 g at the beginning of shelf life, common industry practice is likely to divert this product to alternative route for example, for further downstream processing/cooking into products containing smoked salmon such as pies or quiches. Alternatively, if the product is not diverted, the FBO must have sufficient evidence to demonstrate that the levels of L. monocytogenes will not reach 100 CFU/g at the end of shelf-life. It should, however, be noted that there will be differences between laboratory testing methods used by different FBOs, criteria for release of product at beginning of shelf-life, and for risk management action if L. monocytogenes has been detected. These processes will be examined by and agreed with competent Local Authorities. However, no detection of L. monocytogenes does not guarantee complete absence of the pathogen. It might be present at a level below the test detection limit or the sampling plan might not be sufficient to detect it and as indicated above, any level of L. monocytogenes contamination in RTE smoked fish products may be considered a risk to vulnerable consumers.
Risk to vulnerable consumers
Overall, the number of outbreaks of listeriosis in the UK is very low, even in relation to vulnerable consumers, when examined in the context of the UK consumption data provided in this risk assessment. The over-65 year old population of the UK is 12.5 million (Office for National Statistics), and 6.11% of this would represent over 763,000 over-65s reporting consumption of uncooked smoked fish. The incidence rate of listeriosis per 100,000 population in England and Wales was 0.26 in 2018 and 0.24 in 2019 (most recently available data) which suggests that reported listeriosis infection is rare even amongst more susceptible populations. ACMSF has advised that the qualitative scale can be aligned with an indicative numerical scale for the frequencies of occurrence of risk events and a qualitative low frequency of occurrence has an indicative numerical scale with an assigned frequency of 0.05 - 1.7 cases per 100,000 person years (ACMSF, 2020). However, these groups may not be aware of their increased relative risk of illness following consumption of smoked fish products. Due to the limited information available for milder forms of listeriosis, it has not been possible to understand the level of non-invasive listeriosis experienced by the vulnerable groups considered in this risk assessment.
This risk assessment was produced using a multidimensional model of risk which provides a category for frequency and severity to be taken together as the risk conclusion (see Appendix 2; ACMSF, 2020). On the basis of the evidence presented in this risk assessment, and summarised above, our overall risk conclusion is:
- the frequency of occurrence of invasive listeriosis in the vulnerable population from consumption of cold smoked fish is LOW (for example, rare but does occur)
- the frequency of occurrence of invasive listeriosis in the vulnerable population from consumption of hot smoked fish is VERY LOW for example, very rare but cannot be excluded)
We consider the level of uncertainty for the frequency of occurrence of invasive listeriosis in the vulnerable population from the consumption of hot or cold smoked fish to be MEDIUM. The uncertainty level is largely due to the lack of data on infective doses for L. monocytogenes and the variability in susceptibility to infection amongst different vulnerable groups.
- the severity of illness in vulnerable populations from L. monocytogenes infection is HIGH (for example, severe illness: causing life-threatening or substantial sequelae or illness of long duration)
We consider the level of uncertainty for the severity of illness of listeriosis in the vulnerable population to be LOW. This uncertainty level reflects the large amount of data on the severity of invasive L. monocytogenes infections, particularly within vulnerable groups.
Key uncertainties
The below points contributed to the assignation of a medium uncertainty to the frequency of occurrence of invasive listeriosis:
- there is a lack of data to allow estimation of infectious dose and probability of infection for different vulnerable groups, with dose response models recognised to suffer from uncertainty of the impact of low level exposure on vulnerable populations.
- consumer behaviour around chill storage temperature and use-by date abuse is unknown.
- due to the long incubation period for L. monocytogenes, attributing the source of a case or outbreak as smoked fish can be difficult which may result in smoked fish not being identified as the responsible food vehicle.
- the initial contamination level and how it carries through the food chain will affect the level in the final product.
- variations in processing between FBOs and how those specific conditions may affect L. monocytogenes presence and levels.
- the level of non-invasive listeriosis experienced by the vulnerable groups identified in this risk assessment. This is compounded by the lack of diagnostic investigations for non-invasive listeriosis.
- the extent of awareness of existing government advice. NHS advice (that smoked fish is a food of most concern, and that care should be taken during pregnancy) was recently added to, acknowledging the current incident and advising pregnant consumers to only eat smoked fish products that have been thoroughly cooked. FSA and FSS advice states, that smoked fish is a high-risk product in terms of L. monocytogenes, with recent updates to the website to highlight the on-going incident and advice to consumers at higher risk of serious infection to always thoroughly cook smoked fish products.
- additionally, we note that some smoked fish products do not indicate on the packaging if the smoking process was hot or cold, meaning that consumers may not be aware of the type of processing the product has undergone.
The other contributing sources of uncertainty are:
- uncertainty around the products and species of fish available on retail in the UK (for example, hot smoked, cold smoked, gravad) and the popularity of different products with UK consumers.
- uncertainties around any other factors influencing consumer behaviour with smoked fish RTE products (for example, dietary preferences, which may lead to consuming bigger amounts of this type of product, practices such as leaving the product to warm up to room temperature before consumption, any further cooking prior to consumption etc).
- uncertainties around the difference in risk if smoked fish is used in salad preparations in deli settings
- uncertainties around the understanding of any specific vulnerabilities and the infectious dose for each group or condition which can increase the risk of infection.
It is recognised that some of the uncertainties highlighted above represent variabilities which are distinct from data gaps. For example, the uncertainty around variability in response to exposure to L. monocytogenes experienced by different vulnerable consumers represents both natural variation (for example differing susceptibilities to infection), as well as gaps in data (for example the current lack of understanding as to the different risk relative to the immunocompetent population), and both aspects contribute to the uncertainties which are relevant to the final risk characterisation.
Production processes and risk pathway
L. monocytogenes is a ubiquitous Gram-positive bacterium which occurs naturally in the terrestrial environment, fresh and salt water, livestock manures, decaying plant materials and also in many raw foods associated with these environments (Thomas et al., 2012). Living fish encounter the pathogen in their natural environment (water, soil, decaying vegetation etc), however it has been reported in literature that L. monocytogenes primarily enters food products via cross-contamination in production plants (Jami et al., 2014). For the purposes of this risk assessment, the principal stages of the production of RTE smoked fish products were examined to understand the risk pathway for this organism in this commodity.
Principle stages of the production of RTE smoked fish products and associated risks for Listeria monocytogenes
Harvested fish are transported to primary processors where they are slaughtered and gutted. Slaughtering can occur once the fish have arrived to the primary processor (on shore) or slaughtering can occur in a killing vessel (off shore), where the fish are killed and bled. The culled fish are then transported to the processing premises, where they are gutted and packed (information obtained by FSS as part of investigations of an incident).
Upon reception at the primary processor, the fresh fish are washed to remove the mucus on the fish skin (this mucus can be a source of contamination for L. monocytogenes). Then the fish are eviscerated. During evisceration, contact between flesh and the skin of other fish or waste (viscera, heads) is avoided as the skin, gills and intestines are recognised as the most contaminated parts of the fish. Fish are placed on a conveyor belt with skin against the belt at a speed preventing accumulation of fish to avoid any cross contamination. Correctly carried out early evisceration is crucial to prevent contamination of the flesh with parasites or any bacterial proliferation (incomplete evisceration can be a source of bacterial contamination). The eviscerated fish are then packed and transported (either fresh or frozen to a secondary processor). Note the heads of eviscerated fish are not removed at this point (head on gutted) (European Salmon Smokers Association, 2018).
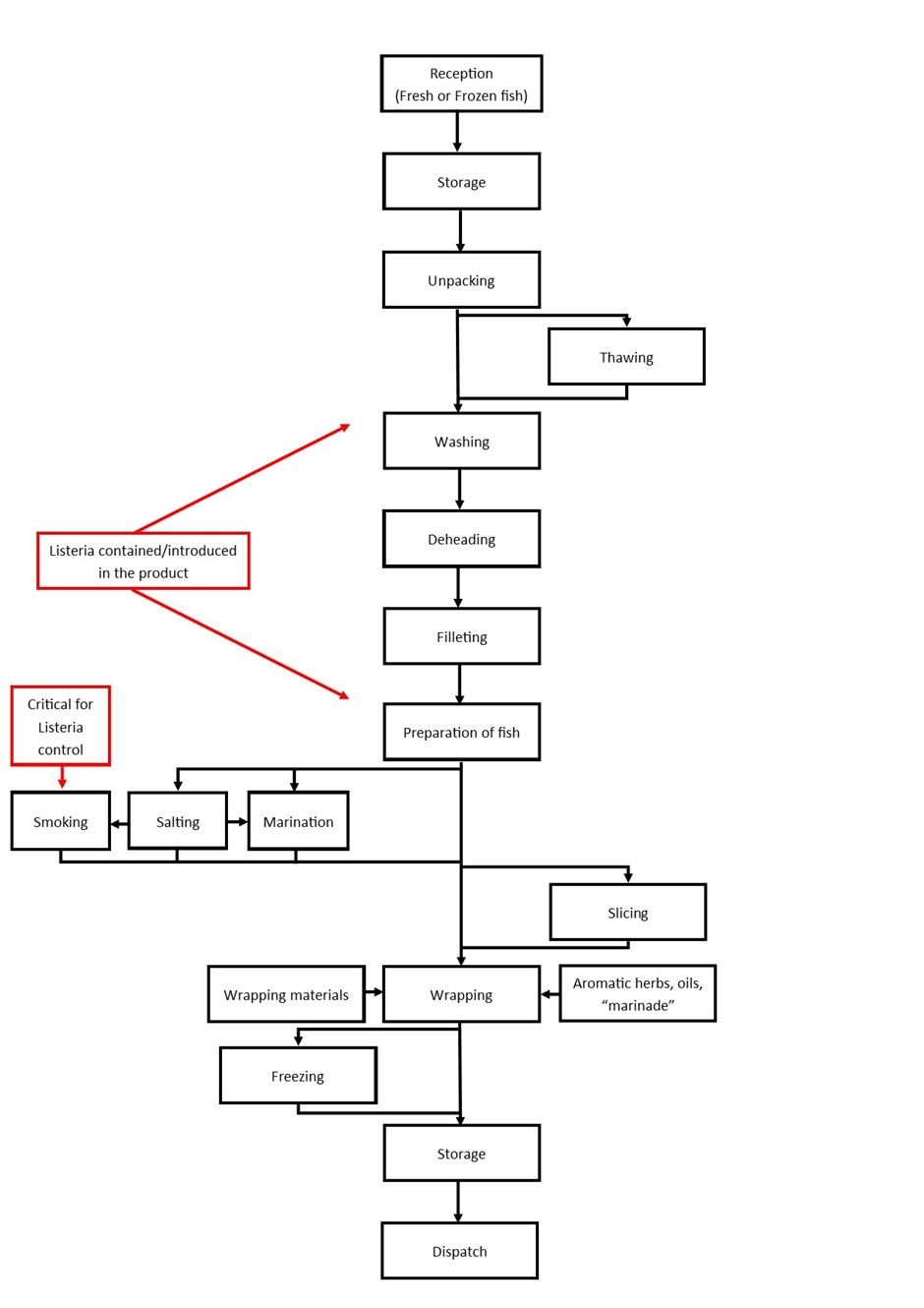
Figure 1 is adapted from The European Salmon Smokers Association guide to good practice for manufacture of smoked fish products, and outlines the main stages in secondary production. It is noted that there are various both smoked and non-smoked RTE fish products which undergo the same general secondary processing steps, and that this adapted figure includes smoked and/or salted and/or marinated fish.
For the purposes of this risk assessment, the critical stages where L. monocytogenes can be introduced and/or controlled during secondary processing are indicated in red in Figure 1. This indicates that L. monocytogenes can be introduced through any stage of secondary processing from “reception” of the gutted fish, “storage”, to “dispatch” to the consumer. L. monocytogenes can be contained within the raw product and proliferate throughout secondary processing. L. monocytogenes contaminated product can cross-contaminate other fish products or contaminate the processing premises. L. monocytogenes can live and persist within the secondary processing environment and contaminate each new batch of product. The stages of “deheading” and “filleting” are where L. monocytogenes on the fish carcass is most likely to cross-contaminate other products, if good manufacturing procedure is not followed correctly (Rotariu et al., 2014; Aalto-Araneda et al., 2019). There is one possible critical control point (CCP), which can result in batch fish being rendered free of L. monocytogenes and that is the heating step process of “hot smoking” (see section 4.1.1.1). Regarding the secondary processing of other RTE smoked fish products, there is not a single processing control step where L. monocytogenes can be completely eliminated.
Figure 1. Principal stages of production for smoked and/or marinated fish products (adapted from European Salmon Smokers Association, 2018) (accessible version)
- Reception (fresh or frozen fish)
- Storage
- Unpacking
- Thawing
- Washing (Listeria contained/introduced in the product)
- Deheading (Listeria contained/introduced in the product)
- Filleting (Listeria contained/introduced in the product)
- Preparation of fish (Listeria contained/introduced in the product)
- Smoking, Salting, Marination (smking is critical for Listeria control)
- Slicing
- Wrapping materials, wrapping, aromic herbs, oils marinade’
- Freezing
- Storage
- Dispatch
Figure 1. Principal stages of production for smoked and/or marinated fish products (adapted from European Salmon Smokers Association, 2018)
As mentioned above, smoked fish processing is split between primary and secondary processing where:
- Primary processing is slaughtering and gutting.
- Secondary processing is filleting, fillet trimming, portioning, producing different cuts such as cutlets, smoking, making ready meals or packing with modified atmosphere.
For the purposes of this risk assessment, the salmon primary and secondary production cycle were examined in further detail. This is due to: 1) information for salmon processing being the most abundantly available evidence and 2) that salmon is the most sold (both fresh and chilled) fish in the UK, which likely reflects consumer preference for this type of fish (Sandercock, 2019; White, 2019).
According to “Salmon Farming Industry Handbook 2019 by MΩWI” the salmon farming production cycle is approximately 3 years. In the first production year, fish eggs are fertilised and fish are grown to 100-150 grams in a controlled freshwater environment. Then the fish are transported to seawater cages, where they continue to grow for 12-24 month until they reach 4-5 kg. Once grown to harvest size, the fish are transported to processing plants where they are slaughtered and gutted. Most salmon is sold to secondary processors gutted and transported on ice in a box (Mowi, 2021).
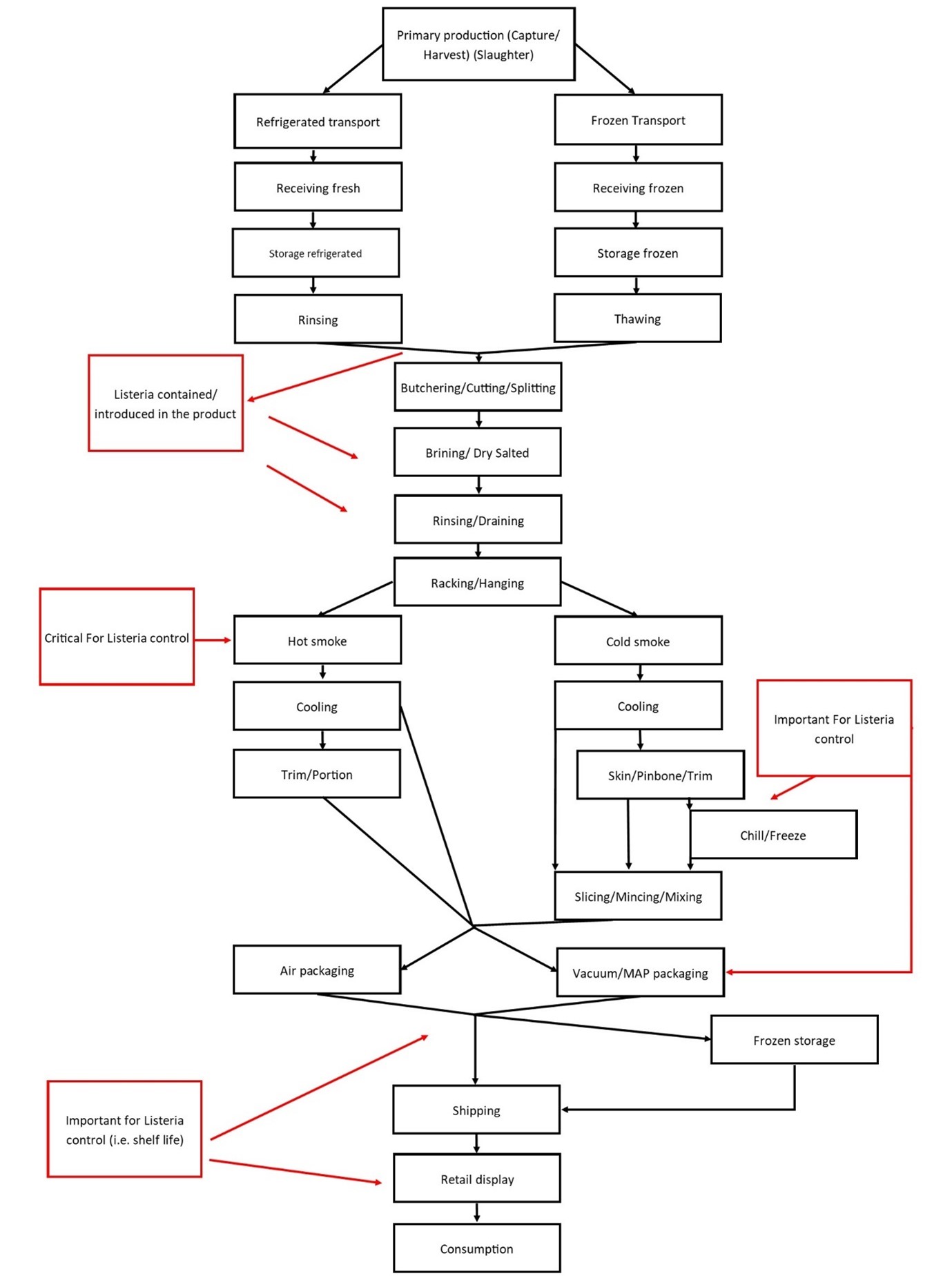
A basic overview flow chart from primary processing through secondary processing and manufacture of cold-smoked and hot-smoked salmon is shown on Figure 2 (Adapted from (FAO, 2006)). The critical stages where L. monocytogenes can be introduced and/or controlled during secondary processing are indicated in red in Figure 2.
It should be noted that there is variation between the specific operations of different FBOs. For example, the time it takes for the cutting, trimming, skinning, and slicing will differ from business to business. Additionally, the salting process varies significantly between different processors – all of the following can be used: dry salting, wet salting, brine injection or submersion in brine. The processes of smoking, for example hot smoking versus cold smoking are completely different (examined in further detail below – see 4.1.1.1 and 4.1.1.2). And each cold smoking and hot smoking process also varies from business to business. Furthermore, the characteristics of the final fish product can also vary significantly between hot smoked and cold smoked products. The hot-smoked product is typically sold and advertised as portions or “chunks” whereas the cold-smoked product is marketed sold as a sliced product or trimmings product. The cold smoked product can also be distributed as whole fillets, which undergo further slicing at the retail establishment. A portion of the hot- and cold-smoked salmon can be also further processed to produce “minces”, “spreads”, and “seafood salads” (FAO, 2006; FAO and WHO, 2006).
L. monocytogenes can be introduced at primary or secondary processing of salmon products. The stages of “butchering/cutting/splitting” are of particular risk for L. monocytogenes where contamination may spread from one contaminated fish to other fish or the processing equipment, if good manufacturing procedure is not followed correctly (Figure 2). Hot smoking offers a critical control step for the elimination of L. monocytogenes (Figure 2). The process of cold smoking could impact the growth and proliferation of L. monocytogenes, but it cannot remove it. Therefore, correctly controlling the cold smoking process and correct shelf-life determination are important for controlling Listeria growth.
Figure 2. An overview from primary processing through secondary processing and manufacture of cold-smoked and hot-smoked salmon (adapted from FAO, 2006) (accessible version)
- Primary production (capture/harvest) (slaughter)
There are two separate processes:
- Refrigerated transport.
- Receiving fresh
- Storage refrigerated.
- Rinsing
- Frozen transport
- Receiving frozen
- Storage frozen
- Thawing
The process then joins up again with the following steps:
1. Butchering/Cutting/Splitting
2. Brining/dry salted
3. Rinsing/Draining
4. Racking/Hanging
Listeria potentially contained/introduced in the product during Brining, dry salted, rinsing and draining stages. The process then separates again for hot smoked and cold smoked fish:
Hot smoke:
- Hot smoke (critical for Listeria control)
- Cooling
- Trim/Portion
- Air packaging or Vacuum/MAP packaging (important for Listeria control and shelf life)
- Frozen storage
- Shipping
- Retail display
- Consumption
Cold smoke:
- Cold smoke
- Cooling
- Skin/Pinbone/Trim
- Chill/Freeze (important for Listeria control)
- Slicing/Mincing/Mixing
- Air packaging or Vacuum/MAP packaging (important for Listeria control and shelf life)
- Frozen storage
- Shipping
- Retail display
- Consumption
Figure 2. An overview from primary processing through secondary processing and manufacture of cold-smoked and hot-smoked salmon (adapted from FAO, 2006)
Control points in the hot smoking process
A typical hot-smoking process uses temperatures of 30-40°C to dry the product, then a hot-smoking period of 2-3 h at 60-70°C, followed by a second drying period (FAO and WHO, 2006). The hot smoking process meets the criteria for a CCP according to the FAO guidelines (FAO, 1997).
If a critical temperature is achieved for a set time across all of the fillets during the hot smoking process, this can result in a batch of fish being rendered completely free of L. monocytogenes (Jemmi and Keusch, 1992; Branciari et al., 2016).
However, the critical temperature has not been definitively determined and there are a number of sources advising different targets. The UK Food Standards Agency, European Salmon Smoker’s Association guidance, FAO guidance, Canadian government and the USDA/US-FDA do not specify a particular temperature that should be achieved for the control of L. monocytogenes in hot smoked fish (FSS, "Safe Smoked Fish Tool"). Food Standards Australia advises L. monocytogenes cannot survive >75°C, (with no specific duration stated) and industry associations such as a working group created by the US National Fisheries Institute and US National Food Processors Association advise that temperature of 145°F (62.8°C) for 30 minutes as sufficient as act as a control point. They do not specifically comment on any effect of smoke on the efficacy of this temperature as a control (National Fisheries Institute and National Food Processors Association, 2002; Food Standards Australia New Zealand, 2016).
The sources cited above agree that unless the level of L. monocytogenes on the fish prior to smoking is extraordinarily high, an adequate hot smoking process should eliminate the pathogen. Thus, any L. monocytogenes present in salmon product after the hot-smoking step is most likely due to recontamination of the product. The effect of this contamination in terms of the frequency of contamination or the levels of Listeria present, depends on the how the product is handled during final manufacturing, distribution, display on retail, and how it is handled by the consumer at home.
Control points in the cold smoking process
A typical cold smoking process involves adding salt and lactic acid to the salmon fillets via injection and/or dry salting. Then there is an equalisation process for 4 hours at maximum of 5°C. Following this, there is a drying period of approx. 5 hours and smoking period for approx. 3.5 hours (note these durations will vary between different businesses). Both drying and smoking are generally performed at temperatures of around 23°-28°C. The salmon is chilled after smoking to a core temperature of 0°C (FAO and WHO, 2006; Porsby et al., 2008; Rasmussen et al., 2017).
There is agreement between both the academic and industry guidance sources cited above that the temperatures used to cold-smoke salmon are insufficient to eliminate L. monocytogenes (FAO and WHO, 2006; Porsby et al., 2008; Rasmussen et al., 2017). Additionally, there are no steps in cold-smoked salmon production after the cold-smoking process that would eliminate L. monocytogenes.
However, the FAO advises that the steps of the cold-smoking process (salting, smoking, drying etc.) can reduce the levels of L. monocytogenes by 90 – 99%, if it was present on the raw salted fish (FAO and WHO, 2006). This is supported by academic studies where, if considered together, the processing steps involved in cold-smoking of salmon are able to reduce the levels of L. monocytogenes but do not eliminate it (Rørvik, 2000; Porsby et al., 2008).
Thus, if any Listeria monocytogenes is present within the product after the cold smoking process it is important that appropriate measures are in place (preventing cross-contamination, chilling, cold storage etc.), and that the shelf life is set correctly, to avoid growth of the microorganism. The frequency of contamination in final product, or the levels of L. monocytogenes present in contaminated product, depends on the food safety management system- how the product is handled during final manufacturing, distribution, display on retail, and how it is handled by the consumer at home.
Unfortunately, there is currently no market data available to indicate what proportion of smoked RTE fish products on retail in the UK are hot smoked vs cold smoked. The section above examined smoked RTE salmon products, as they have been reported to be most sold in the UK (Chilled Seafood in Multiple Retail, 2021). It is also unclear what proportion of other RTE fish are hot or cold smoked. However grey literature sources indicate that the majority of mackerel is hot smoked, whereas trout can be hot or cold smoked (‘Hot smoked, cold smoked - what’s the difference?’, 2019; Hot smoked mackerel; Everything You Need to Know About … Smoked Mackerel).
Other control points
pH and salt content
Although limited, there is a small amount of data describing typical pH and water activity values for smoked seafood sold in the UK (Table 8), obtained during research done for the FSS smoked fish tool (Safe Smoked Fish Tool). In the UK, the salt contents of cold smoked salmon sampled at retail were found to range from 2.2-3.5% and had shelf lives from 10-16 days. An earlier MAFF (1991) study of ‘The microbiological status of some mail order foods’ reported salt concentrations ranging from 3.29-8.11% and shelf lives from 11-20 days. With the reported salt concentrations and available water (aw) typical of smoked fish in the UK, it is considered likely for L. monocytogenes to survive or even grow, as it would not be significantly impacted by these physicochemical properties (Table 8). Regulation 2073/2005 defines characteristics of RTE food which would not support the growth of L. monocytogenes as products with pH ≤ 4.4 or aw ≤ 0.92, products with pH ≤ 5.0 and aw ≤ 0.94, and products with a shelf-life of less than five days. Thus, the UK figures confirm that smoked fish products can support the growth of L. monocytogenes and are unlikely to fall under this definition.
Table 8. Typical properties of various cold smoked fish products sold in the UK
| Product | VP/MAP | NaCI | Shelf life (chilled) | Process | Notes |
|---|---|---|---|---|---|
| Cold smoked salmon |
VP VP or MAP |
Aqueous >3.5% from top to bottom of salmon side Unknown 3% |
16 days 1 to 6 weeks 10 days |
22 to 30 degrees 12 to 24 hours |
UK major multiple International (range) |
| Cold smoked salmon side | VP | 2.2% | >14 days | 22 to 30 degrees 12 to 24 hours | UK Sold on eBay 'Despatch overnight by express carrier' |
| Cold smoked trout |
MAP (10% O2, 50% N2, 40% CO2) |
Aqueous >3.5% from top to bottom of salmon side | 16 days | 22 to 30 degrees 12 to 24 hours | UK Shelf life limited in practice by oragnoleptic quality |
Source: Industry data (published in Peck, Goodburn, Betts, Stringer, 2006). VP is vacuum packed, MAP is modified atmosphere packaging.
Modified atmosphere packaging (MAP) and vacuum packing (VP)
Literature review analysis conducted for the FSS smoked fish tool has demonstrated that naturally present L. monocytogenes can multiply under vacuum pack conditions in smoked fish. Although heavy salting in combination with some smoke residues has been reported to significantly delay growth and possibly even cause partial L. monocytogenes death, vacuum packing in itself is not an effective measure for controlling L. monocytogenes growth or eliminating it entirely during cold storage prior to consumption (Safe Smoked Fish Tool).
Production processes and risk pathway: conclusions
From primary to secondary processing of smoked RTE fish products, there is not a single CCP (apart from effective hot smoking), which fully eliminates L. monocytogenes. If FBOs are following the outlined guidelines by competent authorities and industry associations, the processing steps in the secondary processing of both hot- smoked and cold -smoked salmon should control the growth of L. monocytogenes and maintain it below the legal limit (100 CFU/g) or allow the FBO to demonstrate no detection in 25 grams at the end of secondary processing. This has been previously described as a “hurdle approach”, where multiple controlling factors are implemented to reduce the risk of pathogen growth (FAO, 2006; Tocmo et al., 2014; European Salmon Smokers Association, 2018). However, at any stage from “reception” of the raw fish to its “dispatch” to retail there are points, where the product can either be contaminated with L. monocytogenes or if it naturally contains it, there is possibility for the pathogen to grow during the production steps and during its display at retail.
Consumption data
Consumption data of smoked fish in the UK was determined from the National Diet and Nutrition Survey (NDNS), run jointly by UKHSA and the FSA, using data collected from 2008 to 2019 (National Diet and Nutrition Survey). The NDNS is a dietary survey covering a representative sample of around 1000 people per year in the UK. It is a snapshot over 4 days, so food that is regularly but infrequently consumed may not be reported. Table 9 presents results showing consumption of uncooked smoked fish, including smoked cod, smoked haddock, smoked mackerel, and smoked salmon. The NDNS does not have details on if participants fall within a vulnerable group other than age. Due to the way the data is collected, the adult population figures (table 9) include the overall adult population 16+ without an upper age bracket- for example the 65+ population is included in these figures. As the NDNS specifically excludes pregnant women in its data collection, the consumption habits of women aged 16 to 49 years old were used as a proxy for pregnant women.
Fewer women of child-bearing age report eating smoked fish compared to the general population and they also eat slightly less per day compared to the other groups. Conversely, more participants in the over 65 group report eating smoked fish compared to the general population and they also report eating slightly larger servings. However, the difference in consumption between each vulnerable group included in Table 9 and the general adult population is minimal.
Table 9. Number of people reporting consumption of uncooked smoked fish in the UK and the amount eaten.
| Population Group | % reporting (n/total respondents) | Average g/person/day | Max g/person/day |
|---|---|---|---|
| 16 to 49 (women only) | 4.03% (103/2556) | 73 | 300 |
| 65+ | 6.11% (94/1538) | 82 | 300 |
| Adult population (16+) | 5.28% (404/7653) | 77 | 300 |
Growth and survival of L. monocytogenes
Growth in naturally contaminated fish
Studies using both inoculated and naturally contaminated fish are available, with natural contamination giving a more realistic indication of the potential for survival and growth of L. monocytogenes.
Using a broad Pubmed search of “(Listeria monocytogenes) AND (fish) AND (growth)” just two studies were identified which used naturally contaminated fish to assess growth of L. monocytogenes. Lappi et al. (2004) analysed smoked salmon samples from two processing plants who reported detection of Listeria spp. in 12% and 14% of product respectively in the previous year, however, Listeria spp. was only detected in 5 of the 72 samples tested, and L. monocytogenes in 1 sample. The authors did not comment on this reduction in prevalence, other than that zero samples from plant 3 (where previously 14% of samples had tested positive for Listeria spp.) were positive in this study (Lappi et al., 2004). Each 500g sample was divided into 4 portions with one tested on day zero, and the others vacuum packed, stored at 4°C for 7, 14 or 28 days respectively (Lappi et al., 2004). The one sample for which enumeration was possible (>10 CFU/g) recorded 46 CFU/g at day 7 and 52 CFU/g at day 28, whereas days zero and 14 were recorded at <10 CFU/g, this isolate was identified as Listeria seeligeri. For the one sample where L. monocytogenes was detected, this was only at days 0 and 7 (<2 CFU/g) (Lappi et al., 2004).
Ultimately Lappi et al. (2004) does not provide data to support understanding of the growth of L. monocytogenes in naturally contaminated smoked salmon. Instead, the authors support the findings collated elsewhere in this assessment, that contamination is likely to be at low levels and heterogeneously distributed even within the same piece of fish. In a study of French cold-smoked salmon, Beaufort et al. (2007) sampled 384 vacuum packs within 7 days of processing, then re-vacuum packed the product and stored it at 4°C for 8-15 days, and 8°C for the final 7 days to simulate the likely temperature of a consumer’s fridge. The initial contamination levels of L. monocytogenes were relatively low with the pathogen not detected in 54% of samples (LOD = 0.2 CFU/g), detected at <1 CFU/g in 34% of samples and >1 CFU/g in 12% of samples (Beaufort et al., 2007). The highest recorded level of contamination was 7 CFU/g (Beaufort et al., 2007). At the end of the study L. monocytogenes was not detected in 31% of samples, < 1 CFU/g in 18% of samples and >1 CFU/g in 51% of samples (Beaufort et al., 2007). Over half the samples where L. monocytogenes was detected at >1 CFU/g had levels greater than the legal limit for the end of shelf life (100 CFU/g), and the highest level enumerated was 2800 CFU/g (Beaufort et al., 2007). These results give an indication of the growth of natural contamination over a realistic shelf life and temperature regime. However, they cannot be considered to be truly representative given the wide variation in types of smoked salmon, their processing conditions and product formulation.
Artificial inoculation based growth studies
Scientific literature was examined for artificial inoculation of Listeria monocytogenes growth studies in terms of RTE fish processing conditions and their effect on Listeria growth. The PubMed database was searched using terms “(Listeria monocytogenes) AND (fish) AND (inoculated)”. This produced a total 112 results, out of which 29 were deemed relevant based on information available in the abstract and taken into further consideration. Additional PubMed searches using terms “(Listeria monocytogenes) AND (salmon) AND (inoculated)”, “(Listeria monocytogenes) AND (trout) AND (inoculated)”, “(Listeria monocytogenes) AND (mackerel) AND (inoculated)” identified 5 papers not found in the first search, which were taken into consideration based on information available in the abstract. Overall, 34 papers were examined in detail and appropriate information about the effect of RTE fish processing on the growth of Listeria monocytogenes was extracted. Full text was accessed via the NHS Scotland OpenAthens service.
Although the inoculation studies were carried out in different ways and with different physicochemical parameters, some broad patterns can be pulled out from them. Academic studies using fish inoculated with L. monocytogenes supported the data presented in section 4.1.1.2 using industry data, that appropriate combinations of smoking and brining can reduce the level of contamination in these products. For example, in laboratory conditions it was reported that smoking (liquid smoke) or salting individually had little impact on the level of L. monocytogenes, but that their combined effect significantly reduced the L. monocytogenes population by 1.6 log CFU/g (Neunlist et al., 2005). This was supported by a further study that found that the combination of brining, liquid smoke and drying resulted in a 1-2 log reduction in the level of L. monocytogenes compared to the initial inoculum level (Porsby et al., 2008). The combined importance of heat and smoke in reducing contamination levels was highlighted in a study that found a 10-25 fold reduction in L. monocytogenes from the initial inoculum level when cold smoking took place at 17.2-21.1°C, but that little change in inoculum level was seen when smoking took place at higher temperatures (22.2-30.6°C) (Eklund et al., 1995). The importance of the combination of temperature and smoke was also reported for hot smoked salmon where a minimum hot smoking temperature of 67.2°C was required to inactivate L. monocytogenes in inoculated salmon fillets, and that heating to 82.8°C was required to inactivate L. monocytogenes in the absence of smoke, demonstrating the role that both heat and smoke play in the elimination of L. monocytogenes in hot smoked salmon (Poysky et al., 1997). It is noted that the older studies referenced tend to use initial inoculum levels which are not necessarily representative of natural contamination or prevalence which might be expected in fish processing facilities (Eklund et al., 1995; Poysky et al., 1997). This being taken into consideration, the newer studies using lower levels of initial inoculum, show that the cold smoking conditions (in specific process combinations) can reduce the levels of L. monocytogenes (Neunlist et al., 2005; Porsby et al., 2008).
The impact that consumer behaviour may have on the growth of L. monocytogenes contamination was also illustrated by other studies using inoculated salmon. It was reported that L. monocytogenes inoculated into hot smoked salmon after the smoking process was detected at the same level after 20 days of incubation at 4°C, but where the incubation was at 8-10°C levels significantly increased from the initial inoculum level of 31 most probable number (MPN)/g up to 10,000,000 MPN/g (Jemmi and Keusch, 1992), demonstrating the importance of appropriate fridge temperature in controlling growth of L. monocytogenes in contaminated product. Additionally, it was shown that where smoked salmon samples were inoculated with low (6 CFU/g) or high (600 CFU/g) levels of inoculum, after 4 weeks incubation at 4°C that L. monocytogenes level in some low inoculum samples was equal to or greater than that in high inoculum samples, demonstrating that low levels can multiply substantially (Rørvik, Yndestad and Skjerve, 1991). It was also highlighted that even at high levels of contamination, the sensory quality of the salmon was not affected (Rørvik, Yndestad and Skjerve, 1991), suggesting that consumers are unlikely to be able to detect even very high levels of contamination by any change in the properties of the smoked fish.
Modelling of L. monocytogenes growth in smoked salmon
So far this section has covered the growth of natural contamination of RTE smoked fish products and how industry processing conditions may impact the growth of artificially inoculated L. monocytogenes. This next part will aim to model the growth of L. monocytogenes in cold smoked salmon, under conditions in which a consumer could reasonably be expected to keep it, to help understand the possible growth of contamination after the point of purchase.
To model growth, the online growth curve predictor ComBase was used (ComBase). As cold smoked salmon is typically a chilled product which prescribes storage in refrigerated conditions before consumption, the model assumed storage in a consumer fridge.
There were two independent variables used in the model (to make four models). The first, concentration values of 1 CFU/g (L1) and 10 CFU/g (L10) (Lindqvist & Westöö, 2000) of L. monocytogenes in the product immediately after manufacture were used. (Note: concentration of 1 CFU/g is the lowest possible concentration to use in ComBase). The second, two reasonable consumer behaviours were modelled: consumer 1 (C1) had a median performing fridge temperature of 8.1°C (Brennan et al., 2013) and consumed the product immediately after removing from refrigeration on the last day of shelf life. Consumer 2 (C2) had a fridge which performed in the upper 75% percentile of 8.7°C (Brennan et al., 2013), and consumed the product after allowing it to warm up to room temperature over 30 minutes before consumption, also on the last day of shelf life. The independent variables used for each model are summarised in
Table 10. The independent variables used are based on information from published academic studies and information from FSA “Kitchen life” study (Brennan et al., 2013).
Table 10. The independent variables used to create the four models of L. monocytogenes growth in cold smoked salmon
| Variables | 1 CFU/g (L1) | 10 CFU/g (L10) |
|---|---|---|
| Consumer 1 (fridge 8.1 degrees, eats immediately) (C1) | L1/C1 | L10/C1 |
| Consumer 2 (fridge 8.6 degrees, eats after 30 minutes) (C2) | L1/C2 | L10/C2 |
The dependent variables which were used across all four models were as follows. The physicochemical characteristics of the smoked salmon were taken from a median value from a range of published literature (shown in the Appendix). The available water (aw) was 0.955, the pH was 6.04. The median shelf life used was 16 days (see Appendix 2). To model the time-temperature combinations, the values shown in Table 11 were used (based on data from historical incidents and personal communications with Campden BRI).
Table 11. The time/temperature combinations used in the modelling, factoring in the shelf life of 16 days (384 hours), with differences due to the consumer fridge temperature and behaviours before consumption
| Process | Time (hours) | Time (hours cumulative) | Temperature (degrees celsius) |
|---|---|---|---|
| End manufacture | 0 | 0 | 22 |
| Blast chilled | 0.25 | 0.25 | 4 |
| Transport from manufacturer to retailer display | 48 | 48.25 | 4 |
| On display in retailer | 72 | 120.25 | 5 |
| Consumer picking product, transport from retailer to consumer home | 2 | 122.25 | 22 |
| Storage in consumer fridge | 263.75 (C1) or 263.25 (C2) | 384 (C1) or 383.5 (C2) | 8.1 (C1) or 8.6 (C2) |
| Removal of product to warm up (C2 only) | 0 (C1) or 0.5 (C2) | 384 | 22 |
Table 12. The final concentration of L. monocytogenes indicated by modelling for the consumer behaviour/pathogen concentration value combinations
| - | 1 CFU/g (L1) | 10 CFU/g (L10) |
|---|---|---|
| Consumer 1 (fridge 8.1 degrees, eats immediately) (C1) | 3.03 log CFU/g | 4.02 log CFU/g |
| Consumer 1 (fridge 8.6 degrees, eats after 30 minutes) (C2) | 3.47 log CFU/g | 4.46 log CFU/g |
The modelling (shown in Appendix 1) predicted that, in all four models, the product would have been non-compliant by the end of shelf life (being above 100 CFU/g, or 2 log CFU/g, Table 12). However, the ComBase model does not take into account the effect of smoke or other inhibitory substances, that the organism may be exposed to, thus is not a reliable indicator of levels likely to occur at the end of shelf life. An additional limitation of the model is that it does not take into account the effect of lactic acid bacteria growth and its possible competitive inhibition of L. monocytogenes - another reason why the model can overestimate growth.
Prevalence of L. monocytogenes in RTE Smoked fish
To assess typical prevalence of L. monocytogenes contamination in RTE smoked fish products, a dual approach was used to identify relevant studies. A literature search of Pubmed using the search terms Listeria AND smoked fish was used to identify surveys looking at prevalence of L. monocytogenes in smoked fish products, the date range was limited to 2000 to present. The search term was kept intentionally wide to ensure that any relevant studies could be identified. In total 201 studies were recovered by the search, and 23 of these were identified as potentially relevant. This data was considered alongside UK data identified with the help of FSA and FSS colleagues. Full text was accessed either via publicly available full-text, or via the NHS Scotland OpenAthens service.
Prevalence in cold smoked or hot smoked product
The last large UK wide survey of L. monocytogenes in smoked fish was carried out in 2006 with the results published in 2008 (FSA, 2008). Both cold and hot smoked fish were included in this survey, with L. monocytogenes detected in 17.6% of cold smoked fish samples (236/1344) and 3.4% of hot smoked fish samples (66/1878). The fish species represented in each category were not detailed (FSA, 2008).
Although there are a range of publications reporting prevalence of L. monocytogenes in smoked fish in retail samples from various European countries, only one peer-reviewed paper was identified that specified if the smoked fish product sampled was hot or cold smoked, and provided results for both (Lambertz et al., 2012) (discussed below). In this survey carried out in Sweden in 2010 L. monocytogenes was detected in 15.5% of cold smoked fish samples (n=206), and 1.8% of hot smoked fish samples (n=113) and these figures are broadly similar to those reported for the UK (FSA, 2008; Lambertz et al., 2012).
The data reported by Lambertz et al. (2012) was a combination of both a larger national survey and a smaller set of samples taken to contribute to the EFSA study ‘Analysis of the baseline survey on the prevalence of Listeria monocytogenes in certain ready-to-eat foods in the EU, 2010-2011 Part A: Listeria monocytogenes prevalence estimates’ which was published in 2013 (EFSA, 2013). Countries responding to this survey (26 EU Member States, which included the UK at that time, and 1 non-member) were asked to specify if prevalence data was from cold or hot smoked fish. The prevalence of L. monocytogenes in cold smoked fish was recorded as 17.4% (104/599) and 6.3% in hot smoked fish (33/525), although for an additional 1625 samples the type of smoking was unknown (EFSA, 2013). This data supports the conclusion of the information on production processes presented in section 4.1, that hot smoked fish is less likely to be contaminated with L. monocytogenes, but that it cannot be assumed to be absent, possibly due to contamination following the smoking process.
The Scottish Food Sampling Database (SFSD) collates results from Local Authority testing in Scotland. The results for L. monocytogenes testing in smoked fish (2014-2021) suggests a lower prevalence than the 2008 FSA survey, with 4.7% in cold smoked fish (6 /129 samples) compared to 0.7% for hot smoked fish (2/267 samples) and 2.5% (17/690) where the smoking method was not specified. SFSD can be considered a composite database comprising data from various different sampling programmes including FSS surveillance and Local Authority enforcement and surveillance sampling. The sampling effort is therefore variable from year to year and will also change in terms of how targeted the sample collection is, depending on the type of survey/sampling being conducted and for what reasons. For this reason these data cannot be seen as representative, and results broken down by year have not been presented as, due to the nature of the dataset, any annual trends in prevalence are unlikely to be meaningful.
Effect of fish species on prevalence
The FSA survey did not define which species of smoked fish were included in the UK-wide study (FSA, 2008), but information on species was provided in other publications identified as part of the literature search. However, it is still difficult to summarise if there is any effect of species of fish on the prevalence of L. monocytogenes detected. For example, the prevalence of L. monocytogenes in cold smoked trout was reported to be both higher and lower than that in cold smoked salmon: 26.3% (10/38 samples) compared to 17.7% (16/90), and 0% (0/15 samples) compared to 19% (8/42) (Dominguez, Gomez and Zumalacarregui, 2001; Van Coillie et al., 2004) or L. monocytogenes was reported to be absent in both cold smoked trout and salmon (González-Rodríguez et al., 2002). One issue in identifying any effect of fish species on prevalence of L. monocytogenes is the very small sample numbers included in some studies, and the tendency for the vast majority of samples to be cold-smoked salmon (or salmon where hot or cold smoking is not defined). For example, in their EU-wide survey, EFSA reported that 71% of cold smoked samples were salmon, 9% mackerel, 4.4% herring and 15% other or mixed fish (EFSA, 2013). As illustrated for trout above, where authors indicate higher prevalence of L. monocytogenes in smoked fish products from some species over others, care must be taken to be aware of the sample numbers. For example, Van Coillie et al. (2004) reported that the prevalence of L. monocytogenes in smoked salmon was 19% (8/42 samples) which is broadly consistent with other studies identified, but that 33.3% (6/18 samples) of smoked halibut samples contained detectable levels of L. monocytogenes. However, in their conclusions Van Coillie et al. (2004) indicate that at least 4 of the 6 positive halibut samples come from the same producer over a 4 month period suggesting a persistent strain in one processing facility, as opposed to a particular risk associated with smoked halibut.
For products such as smoked eel where prevalence of 50% was reported (2/4 samples), or swordfish where prevalence of 25% was reported (1/4 samples) no meaningful conclusions can be drawn around the true levels of prevalence in these more unusual smoked fish products due to the low sample size (Uyttendaele et al., 2009; Acciari et al., 2017).
Effect of country or manufacturer on prevalence
As suggested by the study from Van Coillie et al. (2004) above, one supplier experiencing contamination problems can give an artificially high indication of prevalence or give a distorted picture of the real risk consumers are exposed to across smoked fish products from different manufacturers, and this was recognised by other authors. Acciari et al. (2017) report significant differences in prevalence of L. monocytogenes in smoked salmon between both different countries and different manufacturers, with frequency of detection from different manufacturers varying from 0 to 76.9%. Products from twelve different European countries were captured as part of their sampling, and they reported significant differences between prevalence of L. monocytogenes from different countries, although no details were given of countries with higher or lower prevalence so this cannot be accounted for in considering the risk to UK consumers (Acciari et al., 2017). Another study (Swedish) also reported significant variation between prevalence of product from different countries and manufacturers, and highlighted that prevalence was far higher in samples processed overseas (45%) as opposed to domestically (Sweden, 8%), but that these figures were skewed by roughly two-thirds of overseas samples coming from one manufacturer where 50% of samples tested positive (Lambertz et al., 2012). Although Lambertz et al. (2012) stated that this manufacturer was an approved establishment in an EU Member State, no further details are given to help identify the significance of this large manufacturer to the UK consumer. The findings of these studies are supported by the reported outbreaks in Section 3.3, which affected consumers in multiple EU countries, adding weight to the consideration that contamination at one large processor could skew prevalence data and affect a large number of UK consumers.
Additionally heterogeneous distribution of L. monocytogenes contamination within batches was highlighted by a number of authors who tested duplicate sealed packets at the start and end of shelf life, indicating that truly representative sampling of batches is likely to be difficult for businesses to achieve (Uyttendaele et al., 2009; Lambertz et al., 2012; Acciari et al., 2017).
Effect of packaging or further handling on prevalence
Some evidence was found on the effect of packaging or further handling on the prevalence of L. monocytogenes in smoked fish products. Dominguez et al. (2001) reported a prevalence of L. monocytogenes of 17.7% (16/90 samples) in vacuum-packed smoked salmon, but that this rose to 28.5% (12/42 samples) where packaging had been opened prior to sale (for example for sale on a deli counter). Similarly, Uyttendaele et al. (2009) reported detection of L. monocytogenes in 27.8% (25/90) of packaged smoked fish samples, compared with 56.9% prevalence (33/58 samples) in smoked fish used as a raw material in deli-salad preparation, although the breakdown of smoked fish species included in these numbers were not specified. Although a small sample size, Van Coillie et al. (2004) reported that L. monocytogenes was detected in 3 of the 6 smoked salmon salads that they tested, in comparison to 19% (8/42) of packaged smoked salmon samples. A similar pattern to these European findings was recorded in Singapore, where L. monocytogenes was detected in 21.6% (37/171) packaged smoked salmon samples but 86.7% (13/15) of samples taken from unsealed product from salad bars (Chau et al., 2017). The smoked salmon sampled in Singapore originated from Australia, Chile, Denmark, Ireland, Korea, New Zealand, Norway and Scotland (Chau et al., 2017). Although limited in scope and scale, the evidence presented here suggests that the likelihood of detection of L. monocytogenes in smoked fish in deli settings for salad preparation is higher than for vacuum-packed smoked fish, and that this category may represent a further risk to vulnerable consumers. This higher prevalence may be linked to suboptimal storage of the product, additional handling leading to further scope for contamination or lower quality product being diverted into the deli sector, but it is suggested that the initial contamination is likely to originate from manufacture (Dominguez, Gomez and Zumalacarregui, 2001; Van Coillie et al., 2004; Uyttendaele et al., 2009; Chau et al., 2017).
Level of L. monocytogenes in products
Due to differing research questions, and differences in the way data is presented, it is not possible to provide a simple comparison of the frequencies of different levels of L. monocytogenes as presented by different authors. Recognising these difficulties, data has been complied in Table 13 below where authors have provided information on enumeration of samples.
Table 13. Prevalence of L. monocytogenes reported by authors and enumeration of levels >100 CFU/g
| Reference | Country | Species | Detection | Enumberation >100 CFU/g |
|---|---|---|---|---|
| Uyttendaele et al., 2009 | Belgium | 27.8% (25/90) | 4/25 | |
| Acciari et al., 2017 | Italy | 20.2% (157/778) | 26/157 | |
| Dominguez et al., 2001 | Spain | 22.3% (38/170) | 20/38 | |
| Lambertz et al., 2012 | Sweden | Overall 12% (66/558), Cold smoked fish 15.5% (32/206), gravad fish 14.4% (28/194), hot smoked fish 2% (2/113). Plus 4 positive results where smoking process was unknown. | 3/558 | |
| Van Coillie et al., 2004 | Belgium` | 23% (20/87) | 4/20 |
The studies included in Table 13 distinguished where samples had a level > 100 CFU/g, linking this to the requirement specified in Regulation 2073/2005. However, the presentation of results beyond this threshold varied per author. Acciari et al. (2017) reported maximum levels of contamination of 1.3 x 106 at the end of shelf life, and 1.0 x 106 at the start of shelf life (it is unclear if these are for smoked salmon or smoked swordfish samples, although the study included 774 salmon and 4 swordfish samples). Dominguez et al. (2001) reported that of 20 positive samples that contained levels > 100 CFU/g, 18 were between 100 - 1000 CFU/g with the level in one cold smoked salmon sample recorded as 1,100 CFU/g, and one cold smoked trout as 1,700 CFU/g. Lambertz et al. (2012) recorded 3 samples with levels of L. monocytogenes > 100 CFU/g, one cold smoked salmon sample at 130 CFU/g, and 2 gravad salmon samples at 350 and 2500 CFU/g.
- Aalto-Araneda, M. et al. (2019) ‘Processing plant and machinery sanitation and hygiene practices associate with Listeria monocytogenes occurrence in ready-to-eat fish products’, Food Microbiology, 82, pp. 455–464. doi:10.1016/j.fm.2019.03.017.
- Abdelhamed, H. et al. (2019) ‘Validation of Predicted Virulence Factors in Listeria monocytogenes Identified Using Comparative Genomics’, Toxins, 11(9), p. 508. doi:10.3390/toxins11090508.
- Acciari, V.A. et al. (2017) ‘Listeria monocytogenes in Smoked Salmon and Other Smoked Fish at Retail in Italy: Frequency of Contamination and Strain Characterization in Products from Different Manufacturers’, Journal of Food Protection, 80(2), pp. 271–278. doi:10.4315/0362-028X.JFP-15-599.
- ACMSF (2020) Fixed-term group on multidimensional representation of risks (PDF).
- Adak, G.K., Long, S.M. and O’Brien, S.J. (2002) ‘Trends in indigenous foodborne disease and deaths, England and Wales: 1992 to 2000’, Gut, 51(6), pp. 832–841. doi:10.1136/gut.51.6.832.
- Aureli, P. et al. (2000) ‘An outbreak of febrile gastroenteritis associated with corn contaminated by Listeria monocytogenes’, The New England Journal of Medicine, 342(17), pp. 1236–1241. doi:10.1056/NEJM200004273421702.
- Bader, G., Al-Tarawneh, M. and Myers, J. (2016) ‘Review of Prosthetic Joint Infection from Listeria monocytogenes’, Surgical Infections, 17(6), pp. 739–744. doi:10.1089/sur.2016.067.
- Branciari, R. et al. (2016) ‘Thermal inactivation and growth potential of Listeria monocytogenes in smoked tench’, Italian Journal of Food Safety, 5(3). doi:10.4081/ijfs.2016.5974.
- Brennan, M. et al. (2013) Activity Recognition and Temperature Monitoring (ART) Feasibility Study. FS244026 (PDF).
- Chasseignaux, E. et al. (2001) ‘Molecular epidemiology of Listeria monocytogenes isolates collected from the environment, raw meat and raw products in two poultry- and pork-processing plants’, Journal of Applied Microbiology, 91(5), pp. 888–899. doi:10.1046/j.1365-2672.2001.01445.x.
- Chau, M.L. et al. (2017) ‘Microbial survey of ready-to-eat salad ingredients sold at retail reveals the occurrence and the persistence of Listeria monocytogenes Sequence Types 2 and 87 in pre-packed smoked salmon’, BMC Microbiology, 17(1), p. 46. doi:10.1186/s12866-017-0956-z.
- Chilled Seafood in Multiple Retail (2021) Seafish (PDF) (Accessed: 25 May 2022).
- ComBase (no date). (Accessed: 17 May 2022).
- Dalton, C.B. et al. (1997) ‘An Outbreak of Gastroenteritis and Fever Due to Listeria monocytogenes in Milk’, New England Journal of Medicine, 336(2), pp. 100–106. doi:10.1056/NEJM199701093360204.
- Dominguez, C., Gomez, I. and Zumalacarregui, J. (2001) ‘Prevalence and Contamination Levels of Listeria monocytogenes in Smoked Fish and Pâté Sold in Spain’, Journal of Food Protection, 64(12), pp. 2075–2077. doi:10.4315/0362-028X-64.12.2075.
- Drevets, D.A. and Bronze, M.S. (2008) ‘Listeria monocytogenes: epidemiology, human disease, and mechanisms of brain invasion’, FEMS immunology and medical microbiology, 53(2), pp. 151–165. doi:10.1111/j.1574-695X.2008.00404.x.
- EFSA (2013) ‘Analysis of the baseline survey on the prevalence of Listeria monocytogenes in certain ready-to-eat foods in the EU, 2010-2011 Part A: Listeria monocytogenes prevalence estimates’, EFSA Journal, 11(6). (Accessed: 5 May 2022).
- EFSA (2014) ‘Analysis of the baseline survey on the prevalence of Listeria monocytogenes in certain ready-to-eat foods in the EU, 2010–2011 Part B: analysis of factors related to prevalence and exploring compliance’, EFSA Journal, 12(8).
- EFSA (2018) ‘Listeria monocytogenes contamination of ready-to-eat foods and the risk for human health in the EU’, EFSA Journal, 16(1).
- EFSA (2020) United Kingdom- Trends and Sources of Zoonoses and Zoonotic Agents in Foodstuffs, Animals and Feedingstuffs in 2020. (PDF)
- EFSA and ECDC (2018) ‘Multi-country outbreak of Listeria monocytogenes sequence type 8 infections linked to consumption of salmon products’, EFSA Supporting Publications, 15(10), p. 1496E. doi:10.2903/sp.efsa.2018.EN-1496.
- EFSA and ECDC (2019) ‘Multi-country outbreak of Listeria monocytogenes clonal complex 8 infections linked to consumption of cold-smoked fish products’, EFSA Supporting Publications, 16(6), p. 1665E. doi:10.2903/sp.efsa.2019.EN-1665.
- Eicher, C. et al. (2020) ‘Growth Potential of Listeria monocytogenes in Three Different Salmon Products’, p. 13.
- Eklund, M.W. et al. (1995) ‘Incidence and Sources of Listeria monocytogenes in Cold-Smoked Fishery Products and Processing Plants’, Journal of Food Protection, 58(5), pp. 502–508. doi:10.4315/0362-028X-58.5.502.
- Ericsson, H. (1997) ‘An Outbreak of Listeriosis Suspected To Have Been Caused by Rainbow Trout’, 35, p. 4.
- European Salmon Smokers Association (2018) ‘European Guide to Good Practice for Smoked and/or Salted and/or Marinated Fish’. (Accessed: 6 May 2022).
- Everything You Need to Know About … Smoked Mackerel - Fresh Fish Daily (no date). (Accessed: 25 May 2022).
- FAO (1997) Hazard Analysis and Critical Control Point (HACCP) System and Guidelines for its Application. (Accessed: 6 May 2022).
- FAO (2006) The Use of Microbiological Risk Assessment Outputs to Develop Practical Risk Management Strategies: Metrics to improve food safety: Report. Rome, Italy: FAO. (Accessed: 6 May 2022).
- FAO and WHO (2006) ‘Development of Practical Risk Management Strategies based on Microbiological Risk Assessment Outputs’.(PDF)
- Farber, J.M. et al. (2021) ‘Alternative approaches to the risk management of Listeria monocytogenes in low risk foods’, Food Control, 123, p. 107601. doi:10.1016/j.foodcont.2020.107601.
- Farber, J.M. and Peterkin, P.I. (1991) ‘Listeria monocytogenes, a food-borne pathogen’, Microbiological Reviews, 55(3), pp. 476–511. doi:10.1128/mr.55.3.476-511.1991.
- FDA (2003) ‘Quantitative Assessment of Relative Risk to Public Health from Foodborne Listeria monocytogenes Among Selected Categories of Ready-to-Eat Foods’, FDA [Preprint].(Accessed: 21 April 2022).
- Food Standards Australia New Zealand (2016) ‘Imported food risk statement: Processed ready-to-eat finfish and Listeria monocytogenes’. (PDF).
- FSA (2008) ‘A microbiological survey of retail smoked fish with particular reference to the presence of Listeria monocytogenes’.
- FSA (2018) ‘Reducing the risk of vulnerable groups contracting Listeriosis: Guidance for healthcare and social care organisations’. (PDF).
- FSA (2021) ‘Incident Management Plan for Non-Routine Incidents’. (PDF) (Accessed: 15 May 2022).
- FSA (2022) ‘The risk to vulnerable consumers from Listeria monocytogenes in blue cheese’.
- FSS (2018) Reducing the risk of vulnerable groups contracting listeriosis. (PDF) Accessed: 30 May 2022).
- FSS (no date) Safe Smoked Fish Tool. (Accessed: 17 May 2022).
- Fuentes, A. et al. (2010) ‘Physicochemical Characterization of Some Smoked and Marinated Fish Products’, Journal of Food Processing and Preservation, 34(1), pp. 83–103. doi:10.1111/j.1745-4549.2008.00350.x.
- Gahan, C.G.M. and Hill, C. (2005) ‘Gastrointestinal phase of Listeria monocytogenes infection’, Journal of Applied Microbiology, 98(6), pp. 1345–1353. doi:10.1111/j.1365-2672.2005.02559.x.
- Gillesberg Lassen, S. et al. (2016) ‘Two listeria outbreaks caused by smoked fish consumption—using whole-genome sequencing for outbreak investigations’, Clinical Microbiology and Infection, 22(7), pp. 620–624. doi:10.1016/j.cmi.2016.04.017.
- González-Rodríguez, M.-N. et al. (2002) ‘Numbers and types of microorganisms in vacuum-packed cold-smoked freshwater fish at the retail level’, International Journal of Food Microbiology, 77(1–2), pp. 161–168. doi:10.1016/s0168-1605(02)00048-x.
- Guillet, C. et al. (2010) ‘Human Listeriosis Caused by Listeria ivanovii’, Emerging Infectious Diseases, 16(1), pp. 136–138. doi:10.3201/eid1601.091155.
- Health Protection Agency (2009) Guidelines for Assessing the Microbiological Safetyof Ready-to-Eat Foods Placed on the Market, Guidelines for Assessing the Microbiological Safetyof Ready-to-Eat Foods Placed on the Market. (PDF)
- ‘Hot smoked, cold smoked - what’s the difference?’ (2019) Mere Trout, 24 November. (Accessed: 25 May 2022).
- Hot smoked mackerel (no date). (Accessed: 25 May 2022).
- Jami, M. et al. (2014) ‘Listeria monocytogenes in Aquatic Food Products—A Review’, Comprehensive Reviews in Food Science and Food Safety, 13(5), pp. 798–813. doi:10.1111/1541-4337.12092.
- Jemmi, T. and Keusch, A. (1992) ‘Behavior of Listeria monocytogenes during processing and storage of experimentally contaminated hot-smoked trout’, International Journal of Food Microbiology, 15(3), pp. 339–346. doi:10.1016/0168-1605(92)90067-D.
- Kang, J. et al. (2012) ‘Effect of curing method and freeze-thawing on subsequent growth of Listeria monocytogenes on cold-smoked salmon’, Journal of Food Protection, 75(9), pp. 1619–1626. doi:10.4315/0362-028X.JFP-11-561.
- Lachmann, R. et al. (2022) ‘Invasive listeriosis outbreaks and salmon products: a genomic, epidemiological study’, Emerging Microbes & Infections, 0(ja), pp. 1–30. doi:10.1080/22221751.2022.2063075.
- Lambertz, S.T. et al. (2012) ‘Prevalence and level of Listeria monocytogenes in ready-to-eat foods in Sweden 2010’, International Journal of Food Microbiology, 160(1), pp. 24–31. doi:10.1016/j.ijfoodmicro.2012.09.010.
- Lappi, V.R. et al. (2004) ‘Prevalence and growth of Listeria on naturally contaminated smoked salmon over 28 days of storage at 4 degrees C’, Journal of Food Protection, 67(5), pp. 1022–1026. doi:10.4315/0362-028x-67.5.1022.
- Lindqvist, R. and Westöö, A. (2000) ‘Quantitative risk assessment for Listeria monocytogenes in smoked or gravad salmon and rainbow trout in Sweden’, International Journal of Food Microbiology, 58(3), pp. 181–196. doi:10.1016/S0168-1605(00)00272-5.
- Liu, D. et al. (2005) ‘Comparative assessment of acid, alkali and salt tolerance in Listeria monocytogenes virulent and avirulent strains’, FEMS Microbiology Letters, 243(2), pp. 373–378. doi:10.1016/j.femsle.2004.12.025.
- Lopez-Valladares, G., Danielsson-Tham, M.-L. and Tham, W. (2018) ‘Implicated Food Products for Listeriosis and Changes in Serovars of Listeria monocytogenes Affecting Humans in Recent Decades’, Foodborne Pathogens and Disease, 15(7), pp. 387–397. doi:10.1089/fpd.2017.2419.
- Lyhs, U. et al. (2001) ‘Microbiological quality and shelf-life of vacuum-packaged “gravad” rainbow trout stored at 3 and 8 degrees C’, International Journal of Food Microbiology, 70(3), pp. 221–230. doi:10.1016/s0168-1605(01)00548-7.
- Mead, P.S. et al. (1999) ‘Food-related illness and death in the United States’, Emerging Infectious Diseases, 5(5), pp. 607–625. doi:10.3201/eid0505.990502.
- Miettinen, M.K. et al. (1999) ‘Molecular Epidemiology of an Outbreak of Febrile Gastroenteritis Caused by Listeria monocytogenes in Cold-Smoked Rainbow Trout’, Journal of Clinical Microbiology, 37(7), pp. 2358–2360. doi:10.1128/JCM.37.7.2358-2360.1999.
- Miller, A.J. (1992) ‘Combined Water Activity and Solute Effects on Growth and Survival of Listeria monocytogenes Scott A’, Journal of Food Protection, 55(6), pp. 414–418. doi:10.4315/0362-028X-55.6.414.
- Mowi (2021) ‘Salmon Farming Industry Handbook’. (PDF).
- Nakari, U.-M. et al. (2014) ‘Investigation of increased listeriosis revealed two fishery production plants with persistent Listeria contamination in Finland in 2010’, Epidemiology & Infection, 142(11), pp. 2261–2269. doi:10.1017/S095026881300349X.
- National Diet and Nutrition Survey (no date) Food Standards Agency. (Accessed: 15 May 2022).
- National Fisheries Institute and National Food Processors Association (2002) ‘Smoked Seafood Working Group: Listeria monocytogenes Control Manual’. (PDF)
- Neunlist, M.R. et al. (2005) ‘Effect of salting and cold-smoking process on the culturability, viability, and virulence of Listeria monocytogenes strain Scott A’, Journal of Food Protection, 68(1), pp. 85–91. doi:10.4315/0362-028x-68.1.85.
- NHS (2020) Foods to avoid in pregnancy, nhs.uk. (Accessed: 30 May 2022).
- NHS 111 Wales (2022) Pregnancy Guide- Foods to Avoid. (Accessed: 30 May 2022).
- NHS Inform (2022) Eating well in pregnancy. (Accessed: 30 May 2022).
- NIDirect (2022) Foods to avoid in pregnancy. (Accessed: 30 May 2022).
- Office for National Statistics (no date) Population estimates for the UK, England and Wales, Scotland and Northern Ireland: mid-2020. (Accessed: 17 May 2022).
- Orsi, R.H. and Wiedmann, M. (2016) ‘Characteristics and distribution of Listeria spp., including Listeria species newly described since 2009’, Applied Microbiology and Biotechnology, 100, pp. 5273–5287. doi:10.1007/s00253-016-7552-2.
- Peck, M. et al. (2006) Clostridium botulinum in vacuum packed (VP) and modified atmosphere packed (MAP) chilled foods. B13006.
- Pezdirc, K.B. et al. (2012) ‘Listeria monocytogenes and diet during pregnancy; balancing nutrient intake adequacy v. adverse pregnancy outcomes’, Public Health Nutrition, 15(12), pp. 2202–2209. doi:10.1017/S1368980012000717.
- PHE (2017) ‘Listeriosis in England and Wales: Summary for 2017’, p. 16.
- PHE (2018) Listeriosis in England and Wales: summary for 2018, GOV.UK. (Accessed: 20 January 2022).
- PHE (2021) Listeriosis in England and Wales: summary for 2019, GOV.UK. (Accessed: 24 May 2022).
- PHS (2020) Annual summary of Listeria infections, 2019. (Accessed: 22 April 2022).
- Porsby, C.H. et al. (2008) ‘Influence of processing steps in cold-smoked salmon production on survival and growth of persistent and presumed non-persistent Listeria monocytogenes’, International Journal of Food Microbiology, 122(3), pp. 287–295. doi:10.1016/j.ijfoodmicro.2008.01.010.
- Pouillot, R. et al. (2009) ‘Quantitative Risk Assessment of Listeria monocytogenes in French Cold-Smoked Salmon: II. Risk Characterization’, Risk Analysis, 29(6), pp. 806–819. doi:10.1111/j.1539-6924.2008.01200.x.
- Pouillot, R. et al. (2015) ‘Listeria monocytogenes Dose Response Revisited—Incorporating Adjustments for Variability in Strain Virulence and Host Susceptibility’, Risk Analysis, 35(1), pp. 90–108. doi:10.1111/risa.12235.
- Pouillot, R. et al. (2016) ‘Infectious Dose of Listeria monocytogenes in Outbreak Linked to Ice Cream, United States, 2015’, Emerging Infectious Diseases, 22(12). doi:10.3201/eid2212.160165.
- Poysky, F.T. et al. (1997) ‘Inactivation of Listeria monocytogenes on Hot-smoked Salmon by the Interaction of Heat and Smoke or Liquid Smoke †’, Journal of Food Protection, 60(6), pp. 649–654. doi:10.4315/0362-028X-60.6.649.
- Rasmussen, R.R. et al. (2017) ‘Effects of industrial processing on essential elements and regulated and emerging contaminant levels in seafood’, Food and Chemical Toxicology, 104, pp. 85–94. doi:10.1016/j.fct.2017.02.008.
- Ricci, A. et al. (2017) ‘Public health risks associated with hepatitis E virus (HEV) as a food-borne pathogen’, Efsa Journal, 15(7), p. 4886. doi:10.2903/j.efsa.2017.4886.
- Rørvik, L.M. (2000) ‘Listeria monocytogenes in the smoked salmon industry’, International Journal of Food Microbiology, p. 8.
- Rørvik, L.M., Yndestad, M. and Skjerve, E. (1991) ‘Growth of Listeria monocytogenes in vacuum-packed, smoked salmon, during storage at 4° C’, International Journal of Food Microbiology, 14(2), pp. 111–117. doi:10.1016/0168-1605(91)90097-9.
- Rotariu, O. et al. (2014) ‘Smoked salmon industry practices and their association with Listeria monocytogenes’, Food Control, 35(1), pp. 284–292. doi:10.1016/j.foodcont.2013.07.015.
- Sandercock, H. (2019) What lies beneath: fish category report 2019, The Grocer. (Accessed: 30 May 2022).
- Schjørring, S. et al. (2017) ‘Cross-border outbreak of listeriosis caused by cold- smoked salmon, revealed by integrated surveillance and whole genome sequencing (WGS), Denmark and France, 2015 to 2017’, p. 5.
- Tham, W. et al. (2000) ‘Lessons from an outbreak of listeriosis related to vacuum-packed gravad and cold-smoked fish’, International Journal of Food Microbiology, 62(3), pp. 173–175. doi:10.1016/S0168-1605(00)00332-9.
- Thomas, D.J.I. et al. (2012) A review of the published literature and current production and processing practices in smoked fish processing plants with emphasis on contamination by Listeria monocytogenesA. FS425012. (PDF)
- Tocmo, R. et al. (2014) ‘Listeria monocytogenes in Vacuum-Packed Smoked Fish Products: Occurrence, Routes of Contamination, and Potential Intervention Measures’, Comprehensive Reviews in Food Science and Food Safety, 13(2), pp. 172–189. doi:10.1111/1541-4337.12052.
- Townsend, A. et al. (2021) ‘A Systematic Review of Listeria Species and Listeria monocytogenes Prevalence, Persistence, and Diversity throughout the Fresh Produce Supply Chain’, Foods, 10(6), p. 1427. doi:10.3390/foods10061427.
- UK Health Security Agency (no date) Listeria: enhanced surveillance questionnaire, GOV.UK. (Accessed: 17 May 2022).
- Uyttendaele, M. et al. (2009) ‘Prevalence and challenge tests of Listeria monocytogenes in Belgian produced and retailed mayonnaise-based deli-salads, cooked meat products and smoked fish between 2005 and 2007’, International Journal of Food Microbiology, 133(1–2), pp. 94–104. doi:10.1016/j.ijfoodmicro.2009.05.002.
- Van Coillie, E. et al. (2004) ‘Prevalence and Typing of Listeria monocytogenes in Ready-to-Eat Food Products on the Belgian Market’, Journal of Food Protection, 67(11), pp. 2480–2487. doi:10.4315/0362-028X-67.11.2480.
- Walland, J. et al. (2015) ‘Listeria monocytogenes infection in ruminants: Is there a link to the environment, food and human health? A review’, Schweizer Archiv Fur Tierheilkunde, 157(6), pp. 319–328. doi:10.17236/sat00022.
- Warriner, K. and Namvar, A. (2009) ‘What is the hysteria with Listeria?’, Trends in Food Science & Technology, 20(6), pp. 245–254. doi:10.1016/j.tifs.2009.03.008.
- White, K. (2019) Fresh: Meat, Fish & Poultry: Top Products 2019, The Grocer. (Accessed: 30 May 2022).
- WHO (2004) Risk assessment of Listeria monocytogenes in ready-to-eat foods: technical report.
- WHO (2018) Listeriosis, (Accessed: 22 April 2022).
- Zhelyazkov, G. and Stratev, D. (2018) ‘Some Physicochemical Characteristics of Fish Products Sampled from Bulgarian Retail Markets’, Journal of food quality and hazards control, 5(1), pp. 33–36.
Appendix 1
Table A1.1 - Data used to provide the variables used for the ComBase modelling included in section 4.2.1.3
| Product | Packaging | NaCI (%) | Shelf life (days) | aw | pH | Notes | Reference |
|---|---|---|---|---|---|---|---|
| Cold smoked salmon | Vacuum packed | >3.5* | 16 | - | - | UK major multiplier | Peck et al, 2006 |
| Cold smoked salmon | Vacuum packed or modified atmospheric packed | 3 | 7 - 42* | - | - | International (range) | Peck et al, 2006 |
| Cold smoked salmon side | Vacuum packed | 2.2 | >14* | - | - | UK sold on eBay | Peck et al, 2006 |
| Dry cured, cold smoked salmon | Vacuum packed | - | - | 0.931 | 6.07 | raw material sourced from Norway (frozen before manufacture) | Kang et al, 2012 |
| Hand-salted smoked organic Atlantic salmon | - | - | 15 | 0.97 | 6 | Ireland sample collected immediately post manufacture | Eicher et al, 2020 |
| Norwegian smoked salmon (high concentration of sodium lactate) | - | - | 16 | 0.95 | 6 | Norway: sample collected immediately post manufacture | Eicher et al, 2020 |
| Norwegian smoked salmon (low concentration of sodium lactate) | - | - | 16 | 0.96 | 6 | Norway: sample collected immediately post manufacture | Eicher et al, 2020 |
| Smoked salmon | - | 2.16 | - | 0.883 | 5.91 | Bulgaria: at retail | Zhelyazkov and Stratev, 2018 |
| Smoked salmon (brand a) | - | 3.37 | - | 0.95 | 6.3 | Spain: at retail | Fuentes et al, 2010 |
| Smoked salmon (brand b) | - | 2.97 | - | 0.961 | 6.28 | Spain: at retail | Fuentes et al, 2010 |
| Wet cured, cold smoked salmon | Vacuum packed | - | - | 0.962 | 6.14 | Raw material sourced from Norway (frozen before manufacture) | Kang et al, 2012 |
| Median | - | 2.97 | 16a | 0.9555a | 6.04a | - | - |
Figure A1.1: The results of modelling all four conditions, C1/L1 final concentration of L. monocytogenes was 3.03 log CFU/g; C1/L10 final concentration of L. monocytogenes was 4.02 log CFU/g; C2/L1 final concentration of L. monocytogenes was 3.47 log CFU/g; and C2/L10 final concentration of L. monocytogenes was 4.46 log CFU/g.

Appendix 2
This risk characterisation section of this risk assessment followed guidelines produced by the Advisory Committee on the Microbiological Safety of Food (ACMSF, 2020), where the frequency of occurrence and the severity of detriment are considered separately. The tables demonstrating the different levels of risk and uncertainty considered when concluding the risk characterisation are included below.
Table A2.1- A qualitative scale for the frequency of occurrence of foodborne risks.
| Frequency category | Interpretation |
|---|---|
| Negligible | So rare that it does not merit to be considered |
| Very Low | Very rare but cannot be excluded |
| Low | Rare but does occur |
| Medium | Occurs regularly |
| High | Occurs very often |
| Very High | Events occur almost certainly |
Table A2.2 - A qualitative scale for the severity of detriment of foodborne risks.
| Severity category | Interpretation |
|---|---|
| Negligible | No effects, or so mild they do not merit to be considered. |
| Low | Mild illness: not usually life-threatening, usually no sequelae, normally of short duration, symptoms are self-limiting (for example transient diarrhoea) |
| Medium | Moderate illness: incapacitating but not usually life- threatening, sequelae rare, moderate duration (for example diarrhoea requiring hospitalisation) |
| High | Severe illness: causing life-threatening or substantial sequelae or illness of long duration (for example chronic hepatitis) |
Table A2.3 - A qualitative scale for the level of uncertainty in food risk assessment.
| Uncertainty category | Interpretation |
|---|---|
| Low | There are solid and complete data available; strong evidence is provided in multiple references; authors report similar conclusions |
| Medium | There are some but no complete data available; evidence is provided in small number of references; authors report conclusions that vary from one another |
| High | There are scarce or no data; evidence is not provided in references but rather in unpublished reports or based on observations, or personal communication; authors report conclusions that vary considerably between them. |
Revision log
Published: 5 April 2023
Last updated: 5 April 2024