Risk assessment
Qualitative assessment of the risk of SARS-CoV-2 to human health through food exposures to deer in the UK
A risk assessment on the risk to UK consumers from exposure to SARS-CoV-2 via handling and/or consumption of products originating from UK wild/captive deer populations.
Download the full report in PDF:
Risk question
What is the risk to UK consumers from exposure to SARS-CoV-2 via handling and/or consumption of products originating from UK wild/captive deer populations?
In scope
- Deer meat and offal sold at retail
- Deer meat and offal produced by hunters for personal consumption
- Deer meat and offal sold for raw pet food
Out of scope
- Deer meat and offal imported into the UK from other countries
- Exposure from the slaughter or butchery of deer (covered by the UKHSA/PHS risk assessment “Qualitative assessment of the risk of SARS-COV-2 to human health through non-food exposures to deer in the UK” (UKHSA and PHS 2022))
- Deer meat/offal contaminated with SARS-CoV-2 by infected food workers (considered more generally in the FSA’s overarching SARS-CoV-2 risk assessment (FSA 2020))
- Infection in any species other than humans from consumption of SARS-CoV-2 contaminated deer meat or offal
Key assumptions
This risk assessment assumes a scenario where SARS-CoV-2 becomes established in UK deer populations. The risk of this occurring is covered in the risk assessment “What is the risk of SARS-CoV-2 being introduced into the cervid population in Great Britain?” (Defra 2022).
Background
SARS-CoV-2, the coronavirus responsible for the infectious disease COVID-19 (Gorbalenya et al 2020), was first detected in the human population in December 2019 (Zhu et al 2020). It has since spread to become a global pandemic. Previously, two other novel coronaviruses caused illness in the human population. The first, SARS-CoV (for Severe Acute Respiratory Syndrome) was recognised as a new illness in 2004 and the second, MERS-CoV (for Middle East respiratory syndrome) in 2012 (de Wit et al. 2016).
These previous coronavirus outbreaks in humans occurred after bat coronaviruses passed through intermediate hosts (civet cats and camels, respectively) and then transmitted to infect humans (de Wit et al. 2016). SARS-CoV-2 infections in companion animals such as dogs, cats and ferrets and also in captive or farmed animals such as tigers and mink have been observed, likely as spill over events from contact with infected humans (WOAH 2022). There is now a large body of evidence from the United States that SARS-CoV-2 is capable of infecting white-tailed deer and that it can then spread further in the deer population (details in “What is the risk of SARS-CoV-2 being introduced into the cervid population in Great Britain?” (Defra, 2022).
Assuming a worst-case scenario where SARS-CoV-2 is circulating within the UK deer population, this risk assessment was performed to determine whether handling and/or consuming UK-produced deer meat and/or offal may pose a risk of contracting SARS-CoV-2 in humans.
The British Deer Society Deer Distribution Survey 2007 survey shows Roe deer (Capreolus capreolus) being the most widespread. Chinese Water deer (Hydropotes inermis) are the smallest deer population with approximately 700 deer. Other deer populations found in the UK are Red deer (Cervus elaphus), Fallow deer (Dama dama), Muntjac (Muntiacus reevesi) and Sika deer (Cervus nippon). The number of wild deer of all species is estimated at around 2 million, with an annual cull of over 300,000. (Gavin et al., 2019). Farmed deer are principally red deer and make up approximately 27,000 (DEFRA 2021).
Letko et al., (2020) and Walls et al., (2020) show that SARS-CoV-2 requires Angiotensin Converting Enzyme 2 (ACE2) receptors in order to be able to infect a cell; early in the pandemic, Damas et al. had predicted that white-tailed deer may be susceptible to SARS-CoV-2 infection due to their high expression of ACE2 (Damas et al. 2020). The ability of white-tailed deer to be infected has now been confirmed (see Defra, 2022). There is preliminary evidence that UK red, fallow, and roe deer have ACE2 receptors in various tissues, including the nasal passages, the upper respiratory tract, and the digestive tract (APHA, personal communication). It is not currently known whether other proteins necessary for SARS-CoV-2 entry into cells are also present in these deer (uncertainty), although the presence and distribution in tissues of ACE2 in these UK deer populations suggest that they could also shed virus in their nasal secretions and faeces. So far, only one study has been published testing the presence of SARS-CoV-2 in the UK deer population. It analysed serum collected between 2020-2021 from 1,748 UK deer; it found no evidence of SARS-CoV-2 infection in any of the samples (Holding et al. 2022). Additional testing of archived samples, collected between May 2021 and April 2022, by the Animal and Plant Health Agency has identified one UK fallow deer, out of 40 archived deer samples, as seropositive for SARS-CoV-2 (APHA personal communication; Defra, 2022). Another study performed in Germany and Austria tested serum collected from 232 deer, including roe, red, and fallow deer; it found no evidence of SARS-CoV-2 infection in its deer population (Moreira-Soto et al. 2022).
The primary risk pathway is outlined in the figure one.
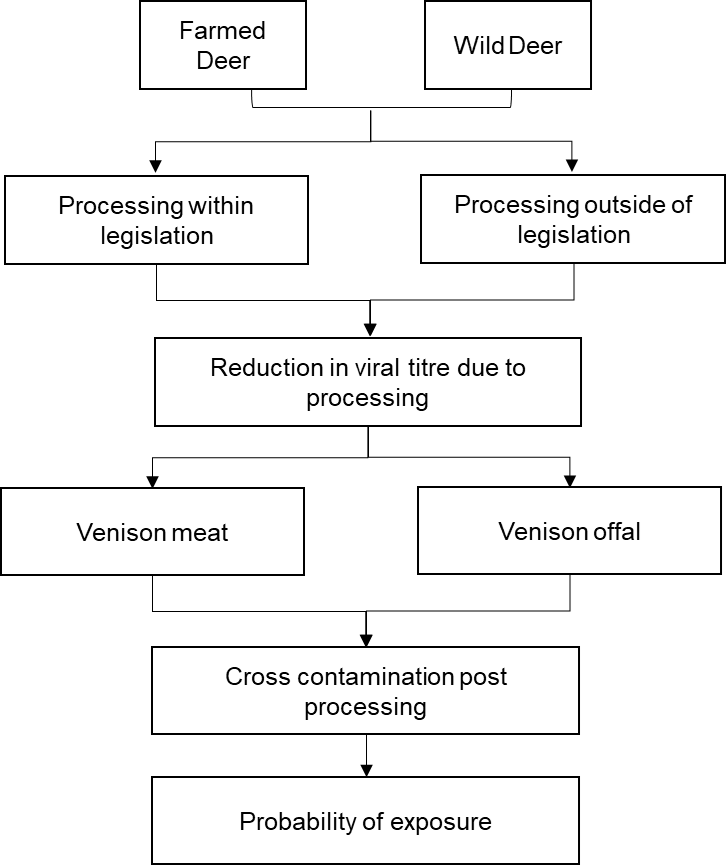
Figure one: Primary risk pathway (text version)
There are two separate pathways; one for wild deer and one for farmed deer.
Farmed Deer
- Processing within legislation
- Reduction in viral titre due to processing
- Venison meat
- Cross contamination post processing
- Probability of exposure
Wild Deer:
- Processing outside of legislation
- Reduction in viral titre due to processing
- Venison offal
- Cross contamination post processing
- Probability of exposure
Preparation and consumption of deer in the UK
All 6 deer species found in the UK can enter the UK foodchain, although the majority (67% based on 2001-2002 venison dealers records) comes from red deer (Gavin et al., 2019; Munro, 2002). Deer meat in the UK can come from farmed or wild deer. Enclosed deer herds in the UK are principally red deer bred on farms or fallow deer within parks, with an estimated 27,000 farmed deer and 40,000 park deer in the UK (DEFRA, 2021; Gavin et al., 2019).
Wild deer are shot by trained hunters and require a hunter’s declaration. They are primarily processed in game handling establishments, which also process other wild game. Deer carcases will undergo visual inspection of the offal and meat during processing removing any deer with visible illness from the foodchain (The Deer Initiative 2009). It is unknown whether there will be visible signs of infection with SARS-CoV-2, for example lesions on the lungs (uncertainty), although this is unlikely and no testing for SARS-CoV-2 will be undertaken. A very small study of 4 white tailed deer reported no overt clinical disease following SARS-CoV-2 infection in any of the inoculated or contact animals during the 21-day experimental period (Palmer et al. 2021). During the evisceration process the green offal (organs associated with the digestive tract) is removed and discarded (often at the site of shooting), and the red offal and head removed and inspected by a trained hunter. The red offal may then enter the foodchain (The Deer Initiative 2009). Several websites provide recipes for offal from hunted deer, focusing mostly on deer heart, liver, tongue, kidney, and testicles ((Pendley, 2019, "Hunter, Angler, Gardener, Cook" 2008, "Field and Stream" 2019). In addition, a Scottish Market Insight report for venison states that 8% of people consuming venison at home have not bought it through retail establishments, and therefore may have hunted and butchered the animals themselves (Scottish Venison 2020), potentially bypassing some of these inspections.
Based on the number of deer slaughtered and processed, either by game handling establishments or slaughter lines, venison in Scotland and England is primarily from hunted wild deer, while venison in Wales and NI has a higher proportion of farmed deer to hunted wild deer (Upadhyay 2018). In the UK there was demand of 160,000 carcases per annum in 2015, with farmed deer making up approximately 3% of this (Gavin et al., 2019).
Based on 2016-2021 data from England, around 50-75,000 wild deer carcases are processed in game handling establishments each year under normal operating conditions (volumes were reduced during COVID measures but are recovering). The numbers of farmed deer processed in these establishments in England during the same time period ranged from 3,200 to 9,800 per year and accounted for between 5%-16% of total carcasses processed (Unpublished data; FSA).
In addition to legally sourced deer, a 2002 report by the British Deer Society (Munro 2002) stated that considerable numbers of deer are poached or illegally sourced (such as via road kill) and subsequently enter the foodchain. It has previously been estimated that hundreds/potentially thousands of animals enter the foodchain by this route (Munro 2002), although the true number is unknown (uncertainty). Additionally, these animals may go into the same game handling establishments and therefore will undergo the same processing prior to consumption (uncertainty).
In 2019-2020, 1,221 tonnes of venison were sold (an increase of 20.1% from the previous year), with 4.7% of households having bought venison (Scottish Venison 2020). 12% of UK consumers reported eating venison at home within the past year while 10% reported eating it out of the home (Scottish Venison 2020). Food consumption data in the UK for venison showed a mean daily consumption of 19.22 g (for all individuals that consume venison). For high level consumers of venison (97.5th percentile), this increases to 187.7 g/day (Unpublished National Diet and Nutrition Survey data, Food Standards Agency). There are no data available on the quantity of deer offal consumed in the UK (uncertainty).
As a meat product, venison will be kept at refrigeration temperatures (≤ 5°C) and may be frozen (-18°C). It is unknown what proportion of venison is frozen prior to consumption, although there is no evidence that refrigeration or freezing will decrease the titres of SARS-CoV-2 on meat or meat products within the shelf-life of the product.
Venison can be consumed a number of ways. These can include:
- Composite foods for example, pies, sausages, stews, etc. These usually require thorough / slow cooking of the meat prior to consumption which is highly likely to completely inactivate any virus present on or within the meat.
- Joints or steaks. The outside surface will be thoroughly cooked, but the inside may still be consumed rare or less than thoroughly cooked.
- There is some evidence that venison can also be prepared tartare (raw) ("Hunter-Eater", 2013; "Hunter, Angler, Gardener, Cook", 2013).
The proportion of venison sold in the UK that will be consumed less than thoroughly cooked or raw is unknown (uncertainty).
SARS-CoV-2 presence in muscle and organs
In one of the studies where deer were experimentally inoculated with SARS-CoV-2, the researchers investigated the presence of the virus in different tissues throughout the body (Palmer et al. 2021). No viral RNA was detected in sections of lung, kidney, brain, intestine, or mesenteric lymph nodes; muscles of the deer were not tested (Palmer et al. 2021). Whether muscle tissue (and therefore meat) can be infected with SARS-CoV-2 has not been well studied; similar coronaviruses have not been looked for in the muscles of mammals. SARS was not found within human muscles when it was found in other tissues (Ding et al. 2004), and more recent studies in humans determined ACE2 expression levels in muscle tissue were low (Li et al. 2020). From the very limited data on experimentally infected animals, it is thought to be unlikely that camel meat and internal organs will be infected by MERS‐CoV, though further studies are needed to confirm this (Hemida et al. 2017).
Factors affecting SARS-CoV-2 survival
SARS-CoV-2 is no more resistant to heat than other viruses (WHO 2020). Research has shown SARS-CoV-2 (in liquid culture) is inactivated in under 5 minutes at 70°C and under 30 minutes at 56°C (Chin et al. 2020). This means that thorough cooking of venison meat would remove the risk of infection from meat. It is unclear whether less than thorough cooking of venison would completely inactivate infectious SARS-CoV-2 (uncertainty).
SARS-CoV-2 is susceptible to biocides used in the food production environment and consumer kitchens (Rowan, Meade, and Garvey 2021). Therefore, the likelihood of SARS-CoV-2 cross-contamination can be reduced using standard factory or household disinfectants and by following good hygiene practices.
Research has shown SARS-CoV-2 is relatively stable at chilled temperatures when in liquid broth (Chin et al. 2020). Similar results have been seen by (Fisher et al. 2021) who assessed the survival of SARS-CoV-2 on refrigerated and frozen chicken, salmon and pork pieces over 3 weeks. They found the titre and infectivity of SARS-CoV-2 remained stable at 4°C, –20°C and –80°C for the duration of the experiment. No studies have been published assessing the survival of SARS-CoV-2 on venison at chilled or frozen temperatures (uncertainty). Assuming it is similar to other meats, the cold chain of venison may allow the survival of SARS-CoV-2 in infected meat.
SARS-CoV-2 infection via handling of raw meat
If deer meat or offal is infected with SARS-CoV-2, then handling of the raw meat may allow for cross-contamination of surfaces; this may serve as a potential source of infection if people touch the contaminated surfaces and then touch a mucous membrane. As there currently is no evidence of SARS-CoV-2 presence in deer meat or offal, viral levels from such cross-contamination events and thus the potential dose encountered are not known (uncertainty). Two different risk assessments considering the risk of cross-contamination with food items infected with SARS-CoV-2 concluded the risk was negligible to very low (FSA 2020; Locas et al. 2022). Practicing good hygiene during food preparation will help reduce the potential risk of acquiring SARS-CoV-2 from contaminated meat/offal (FSA 2020; Locas et al. 2022; USDA Animal and Plant Health Inspection Service 2021).
SARS-CoV-2 infection from handling raw pet food
Outside personal consumption, another reason consumers may handle raw meat is as a food source for companion animals. Raw pet food containing deer meat and offal are available for purchase in the UK. It is not known what proportion of the raw pet food market may consist of deer meat and offal (uncertainty). The similarity between the deer population used to produce raw pet food and the population of deer that enters the food chain for human consumption is unknown. However, given that animal by-products used in the production of raw pet food are assumed fit for human consumption then deer entering both food chains are likely to be similar. Guidelines around storage and hygiene, related to handling raw pet food, recommend it be kept frozen until use and anything that comes into contact with the product (like hands, surfaces, utensils, etc), should be washed to prevent any cross-contamination (PHE and APHA 2018). As noted above, freezing is unlikely to reduce viral load. Raw pet food would not undergo any heat treatment that would reduce viral titres. Given the lack of evidence on whether SARS-CoV-2 infects muscle tissue and if ingesting the virus can lead to active infection, the risk from handling raw deer meat and offal produced as raw pet food is unlikely to serve as a source of human infection.
SARS-CoV-2 infection via food
SARS-CoV-2 requires the presence of the Angiotensin-converting enzyme 2 (ACE2) receptor to infect a cell ((Letko, Marzi, and Munster 2020); Walls et al., 2020)). This receptor is present in various human tissues – most importantly for infection through food are the oral mucosa, stomach, small intestine, and colon (Hamming et al. 2004). In addition, the pH of human stomach acid is between 1.5 and 3.5, and the survival of SARS-CoV-2 is unknown below pH 3 (uncertainty). However, studies on SARS-CoV-1 suggest that the virus is likely to be inactivated by the pHs found in large parts of the human digestive system (Darnell et al. 2004) and therefore infection via the oral mucosa may present the most credible route of infection during ingestion of contaminated foodstuffs. Certain medications may theoretically affect this potential for infection; for example, individuals undergoing treatment involving proton pump inhibitor medication are likely to have reduced stomach acidity with potential consequences for viral inactivation during digestion, although the effect of this on the likelihood of infection via the GI route has not been proven (uncertainty).
There is little evidence that the oral / gastrointestinal route can lead to infection from SARS-CoV-2. One study has reported the detection of SARS-CoV-2 RNA in gastrointestinal tissues (Xiao et al. 2020), although there have been no studies that have proven oral transmission of SARS-CoV-2 (uncertainty). A previous FSA risk assessment on the risk of food or food contact materials and surfaces being a source or transmission route of SARS-CoV-2 for UK consumers concluded that the probability that UK consumers will receive potentially infectious exposures of SARS-CoV-2 via the consumption of food is Negligible (so rare that it does not merit to be considered) for foods of animal origin where the meat is contaminated due to infection of the animal, although the uncertainty was high due to the recent emergence of the virus (FSA 2020). This has been supported by several other risk assessments undertaken across the world ((CDC 2020), (US EPA 2020)). Additionally, a qualitative study showing the likelihood of exposure to SARS-CoV-2 via the food chain showed a negligible to very low risk throughout the food chain, but noted the lack of comprehensive evidence that ingestion of viral particles would be a route of infection for SARS-CoV-2 (Locas et al. 2022).
The symptoms of COVID-19 include headaches, runny nose, sore throat and persistent cough, although vary depending on such things as vaccination status of the individual infected and the variant of SARS-CoV-2. The severity of symptoms varies, with most people experiencing mild to moderate severity disease and recovering without requiring special treatment. Some will experience severe disease requiring medical intervention. This is more likely to occur in older people or those with underlying comorbidities such as cardiovascular or respiratory disease, or cancers; however, anyone can have severe COVID-19 (WHO 2022). In addition, some people infected will go on to experience long COVID; although most will recover from this within 12 weeks, some will experience it for much longer (NHS 2021).
There have been 22,241,858 confirmed positive cases of COVID-19 in the UK since the virus was first described (data to 1st of December 2022, (GOV.UK). Of these, there were 993,749 hospitalisations and 209,685 deaths with COVID-19 on the death certificate (data to 1st of December 2022, (GOV.UK). There has been widespread vaccination in the UK, with 53,813,491 people having received at least one dose, 50,762,968 having received two doses and 40,373,987 of those having also received a booster or third vaccine (data to 1st of December 2022, (GOV.UK).
Even if deer are infected, there is little evidence that viable virus would be present in the muscle tissue (uncertainty). Levels of virus in the different deer organs consumed as offal is also unknown (uncertainty). Most deer meat will likely be cooked (uncertainty), reducing the number of any viable virus present in the meat. Cross-contamination of surfaces prior to cooking is a concern, although risk assessments determined the risk of acquiring COVID-19 from cross-contamination from food sources to be negligible to very low (Locas et al. 2022). Finally, as SARS-CoV-2 is a respiratory illness, the ability to be infected from ingestion of virus particles is not currently known (uncertainty).
Despite the high prevalence of SARS-CoV-2 in some deer populations in the United States, the USDA still indicates there “is no evidence that people can get COVID-19 by preparing or eating meat from an animal infected with SARS-CoV-2, including wild game meat” (USDA Animal and Plant Health Inspection Service 2021). Similarly, several risk assessments and literature reviews from different organisations have not identified any evidence for infection from SARS-CoV-2 from food (BfR (German Federal Institute for Risk Assessment) 2022; FSA 2020; ICMSF 2020; New Zealand Food Safety Science and Research Centre 2022). Two of these have updated their evidence for 2022 and, despite over two years of the global SARS-CoV-2 pandemic, still did not find evidence for infections of SARS-CoV-2 from food (BfR (German Federal Institute for Risk Assessment) 2022; New Zealand Food Safety Science and Research Centre 2022)
Given the above, the risk of contracting COVID-19 associated with handling or consuming UK-produced deer meat and offal is negligible (so rare that it does not merit to be considered) with a medium uncertainty. This uncertainty is primarily due to the lack of data on the presence of viable virus in deer meat and offal and ability of SARS-CoV-2 to infect via the oral route, aka through the ingestion of contaminated food.
Uncertainties
- Whether deer meat / musculature / offal may have viable virus associated with it when a deer is actively infected with SARS-CoV-2 and, if so, at what level
- Whether SARS-CoV-2 be transmitted to people via the oral route and, if so, how this is affected by dose and vehicle
- Whether there are visible signs of infection with SARS-CoV-2 in UK deer and if these would be sufficient for removal of the carcass from the human foodchain via inspection to be likely
- Proportion of deer meat in the UK eaten less than thoroughly cooked
- Quantity of deer offal consumed in the UK and typical preparation
- Proportion of the UK raw pet food market made up of UK-produced deer meat and offal
- BfR (German Federal Institute for Risk Assessment). 2022. ‘Can SARS-CoV-2 Be Transmitted Via Food And Objects?’
- CDC. 2020. ‘Information about Drinking Water, Treated Recreational Water, and Wastewater’. Centers for Disease Control and Prevention. 11 February 2020.
- Chin, Alex W. H., Julie T. S. Chu, Mahen R. A. Perera, Kenrie P. Y. Hui, Hui-Ling Yen, Michael C. W. Chan, Malik Peiris, and Leo L. M. Poon. 2020. ‘Stability of SARS-CoV-2 in Different Environmental Conditions’. The Lancet Microbe 0 (0). https://doi.org/10.1016/S2666-5247(20)30003-3.
- Damas, Joana, Graham M. Hughes, Kathleen C. Keough, Corrie A. Painter, Nicole S. Persky, Marco Corbo, Michael Hiller, et al. 2020. ‘Broad Host Range of SARS-CoV-2 Predicted by Comparative and Structural Analysis of ACE2 in Vertebrates’. Proceedings of the National Academy of Sciences of the United States of America 117 (36): 22311–22. https://doi.org/10.1073/pnas.2010146117.
- Darnell, Miriam E. R., Kanta Subbarao, Stephen M. Feinstone, and Deborah R. Taylor. 2004. ‘Inactivation of the Coronavirus That Induces Severe Acute Respiratory Syndrome, SARS-CoV’. Journal of Virological Methods 121 (1): 85–91. https://doi.org/10.1016/j.jviromet.2004.06.006.
- ‘Deer Heart Recipes, Deer Liver Recipes, Venison Offal Recipes’. 2008. Hunter Angler Gardener Cook. 25 January 2008.
- DEFRA. 2021. ‘Farming Statistics - Land Use, Livestock Populations and Agricultural Workforce as at 1 June 2021, England’. GOV.UK. 28 October 2021.
- Defra. 2022. ‘What Is the Risk of SARS-CoV-2 Being Introduced into the Cervid Population in Great Britain?’
- Ding, Yanqing, Li He, Qingling Zhang, Zhongxi Huang, Xiaoyan Che, Jinlin Hou, Huijun Wang, et al. 2004. ‘Organ Distribution of Severe Acute Respiratory Syndrome (SARS) Associated Coronavirus (SARS-CoV) in SARS Patients: Implications for Pathogenesis and Virus Transmission Pathways’. The Journal of Pathology 203 (2): 622–30. https://doi.org/10.1002/path.1560.
- Farm Animal Welfare Commission. 2013. ‘FAWC Opinion on the Welfare of Farmed and Park Deer’ (PDF).
- Fisher, Dale, Alan Reilly, Adrian Kang Eng Zheng, Alex Cook, and Danielle Anderson. 2021. ‘Seeding of Outbreaks of COVID-19 by Contaminated Fresh and Frozen Food’. bioRxiv. https://doi.org/10.1101/2020.08.17.255166.
- FSA. 2020. ‘Qualitative Risk Assessment on the Risk of Food or Food Contact Materials as a Transmission Route for SARS-CoV-2’. Food Standards Agency. 12 June 2020.
- Gavin, Christine, Davin Henderson, Sylvie L. Benestad, Marion Simmons, and Amie Adkin. 2019a. ‘Estimating the Amount of Chronic Wasting Disease Infectivity Passing through Abattoirs and Field Slaughter’. Preventive Veterinary Medicine 166 (May): 28–38. https://doi.org/10.1016/j.prevetmed.2019.02.016.
- GOV.UK. n.d. ‘Cases in the UK | Coronavirus in the UK’. Accessed 1 March 2022.
- Hamming, I., W. Timens, M. L. C. Bulthuis, A. T. Lely, G. J. Navis, and H. van Goor. 2004. ‘Tissue Distribution of ACE2 Protein, the Functional Receptor for SARS Coronavirus. A First Step in Understanding SARS Pathogenesis’. The Journal of Pathology 203 (2): 631–37. https://doi.org/10.1002/path.1570.
- Hemida, M. G., A. Elmoslemany, F. Al‐Hizab, A. Alnaeem, F. Almathen, B. Faye, D. K. W. Chu, R. A. P. M. Perera, and M. Peiris. 2017. ‘Dromedary Camels and the Transmission of Middle East Respiratory Syndrome Coronavirus (MERS‐CoV)’. Transboundary and Emerging Diseases 64 (2): 344–53. https://doi.org/10.1111/tbed.12401.
- Holding, Maya, Ashley David Otter, Stuart Dowall, Katsuhisa Takumi, Bethany Hicks, Tom Coleman, Georgia Hemingway, et al. 2022. ‘Screening of Wild Deer Populations for Exposure to SARS-CoV-2 in the United Kingdom, 2020–2021’. Transboundary and Emerging Diseases n/a (n/a). https://doi.org/10.1111/tbed.14534.
- ICMSF. 2020. ‘ICMSF Opinion on SARS-CoV-2 and Its Relationship to Food Safety’ (PDF).
- Letko, Michael, Andrea Marzi, and Vincent Munster. 2020. ‘Functional Assessment of Cell Entry and Receptor Usage for SARS-CoV-2 and Other Lineage B Betacoronaviruses’. Nature Microbiology 5 (4): 562–69. https://doi.org/10.1038/s41564-020-0688-y.
- Li, Meng-Yuan, Lin Li, Yue Zhang, and Xiao-Sheng Wang. 2020. ‘Expression of the SARS-CoV-2 Cell Receptor Gene ACE2 in a Wide Variety of Human Tissues’. Infectious Diseases of Poverty 9 (1): 45. https://doi.org/10.1186/s40249-020-00662-x.
- Locas, Annie, Julie Brassard, Megan Rose-Martel, Dominic Lambert, Alyssa Green, Anne Deckert, and Michelle Illing. 2022. ‘Comprehensive Risk Pathway of the Qualitative Likelihood of Human Exposure to Severe Acute Respiratory Syndrome Coronavirus 2 from the Food Chain’ 85 (1). https://doi.org/10.4315/JFP-21-218.
- Moreira-Soto, Andres, Christian Walzer, Gábor Á Czirják, Martin H. Richter, Stephen F. Marino, Annika Posautz, Pau De Yebra Rodo, Gayle K. McEwen, Jan Felix Drexler, and Alex D. Greenwood. 2022. ‘Serological Evidence That SARS-CoV-2 Has Not Emerged in Deer in Germany or Austria during the COVID-19 Pandemic’. Microorganisms 10 (4): 748. https://doi.org/10.3390/microorganisms10040748.
- Munro, RANALD. 2002. ‘Report on the Deer Industry in Great Britain’ (PDF).
- New Zealand Food Safety Science and Research Centre. 2022. ‘POTENTIAL FOR FOODBORNE TRANSMISSION OF COVID-19: LITERATURE REVIEW UPDATE VERSION 7’ (PDF). 2022.
- NHS. 2021. ‘Long-Term Effects of Coronavirus (Long COVID)’. Nhs.Uk. 7 January 2021.
- Palmer, Mitchell V., Mathias Martins, Shollie Falkenberg, Alexandra Buckley, Leonardo C. Caserta, Patrick K. Mitchell, Eric D. Cassmann, et al. 2021. ‘Susceptibility of White-Tailed Deer (Odocoileus Virginianus) to SARS-CoV-2’. Journal of Virology, March. https://doi.org/10.1128/JVI.00083-21.
- Pendley, Michael. 2019. ‘How to Cook Deer Organs & Offal - Petersen’s Hunting’. Petersens Hunting. 3 October 2019.
- PHE, and APHA. 2018. ‘Raw Pet Foods: Handling and Preventing Infection’. GOV.UK. 17 October 2018.
- ‘Recipe: Venison Tartare’. 2013. Hunter-Eater (blog). 13 November 2013.
- Rowan, Neil J., Elaine Meade, and Mary Garvey. 2021. ‘Efficacy of Frontline Chemical Biocides and Disinfection Approaches for Inactivating SARS-CoV-2 Variants of Concern That Cause Coronavirus Disease with the Emergence of Opportunities for Green Eco-Solutions’. Current Opinion in Environmental Science & Health 23 (October): 100290. https://doi.org/10.1016/j.coesh.2021.100290.
- Scottish Venison. 2020. ‘UK Venison Facts 2019-2020’ (PDF), April.
- ‘The Complete Guide to Cooking and Eating Venison Offal’. 2019. Field & Stream (blog). 25 November 2019.
- The Deer Initiative. 2009. ‘Carcass Inspection - Meat Hygiene Best Practice Guides’. 20 February 2009.
- UKHSA and PHS. 2022. ‘Qualitative Assessment of the Risk of SARS-COV-2 to Human Health through Non-Food Exposures to Deer in the UK’.
- Upadhyay, Manisha. 2018. ‘Risk of Infection from Chronic Wasting Disease Prions and Atypical Chronic Wasting Disease Prions via Consuming Cervid Meat’ (PDF), June.
- US EPA, OA. 2020. ‘Coronavirus and Drinking Water and Wastewater’. Overviews and Factsheets. 11 March 2020.
- USDA Animal and Plant Health Inspection Service. 2021. ‘Questions and Answers: Results of Study on SARS-CoV2 in White-Tailed Deer’, 2.
- ‘Venison Tartare Recipe - How to Safely Make Venison Tartare’. 2013. Hunter Angler Gardener Cook. 15 May 2013.
- Walls, Alexandra C., Young-Jun Park, M. Alejandra Tortorici, Abigail Wall, Andrew T. McGuire, and David Veesler. 2020. ‘Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein’. Cell 181 (2): 281-292.e6. https://doi.org/10.1016/j.cell.2020.02.058.
- WHO. 2020. ‘Coronavirus Disease (COVID-19): Food Safety for Consumers’. 14 August 2020.
- WHO. 2022. ‘Coronavirus’. 2022.
- Wit, Emmie de, Neeltje van Doremalen, Darryl Falzarano, and Vincent J. Munster. 2016. ‘SARS and MERS: Recent Insights into Emerging Coronaviruses’. Nature Reviews Microbiology 14 (8): 523–34. https://doi.org/10.1038/nrmicro.2016.81.
- WOAH. 2022. ‘COVID-19’. WOAH - World Organisation for Animal Health (blog). 2022.
- Xiao, Fei, Meiwen Tang, Xiaobin Zheng, Chunna Li, Jianzhong He, Zhongsi Hong, Siwen Huang, et al. 2020. ‘Evidence for Gastrointestinal Infection of SARS-CoV-2’. MedRxiv, February, 2020.02.17.20023721. https://doi.org/10.1101/2020.02.17.20023721.
This risk assessment was produced by the FSA at the request of the Human Animal Infections and Risk Surveillance group.
Thanks to the following for providing data, etc:
- Dr. Josheph Shavila (Food Standards Agency)
- Emma French (Food Standards Agency)
- Kelly Carmonday (Food Standards Agency)
- Richard Playfair (Scottish Venison)
Interpretation of probability categories used in this risk assessment.
Table from ACMSF (ACM/1065) adapted from EFSA 2006 modified from OIE 2004.
| Probability category | Interpretation |
|---|---|
| Negligible | So rare that it does not merit to be considered |
| Very low | Very rare but cannot be excluded |
| Low | Rare, but does occur |
| Medium | Occurs regularly |
| High | Occurs very often |
| Very high | Events occur almost certainly |
Qualitative categories for expressing uncertainty in relation to qualitative risk estimates
Table from ACMSF (ACM/1065) adapted from EFSA 2006.
| Uncertainty category | Interpretation |
|---|---|
| Low | There are solid and complete data available; strong evidence is provided in multiple references; authors report similar conclusions |
| Medium | There are some but no complete data available; evidence is provided in a small number of references; authors report conclusions that vary from one another |
| High | There are scarce or no data available; evidence is not provided in references but rather in unpublished reports or based on observations, or personal communication; authors report conclusions that vary considerably between them |